
![]()
Dilated Cardiomyopathy (DCM)
There are no specific ECG features unique to DCM, however the ECG is usually NOT normal.
Common ECG associations with DCM
- Left atrial enlargement (may progress to atrial fibrillation)
- Biatrial enlargement
- Left ventricular hypertrophy or biventricular enlargement
- Left bundle branch block (RBBB can also occur)
- Left axis deviation
- Poor R-wave progression with QS complexes in V1-4 (“pseudo-infarction” pattern)
- Frequent ventricular ectopics and ventricular bigeminy (seen with severe DCM)
- Ventricular dysrhythmias (VT/VF)
- The most common ECG abnormalities are those associated with atrial and ventricular hypertrophy — typically, left-sided changes are seen but there may be signs of biatrial or biventricular hypertrophy
- Interventricular conduction delays (e.g. LBBB) occur due to cardiac dilatation
- Diffuse myocardial fibrosis may lead to reduced voltage QRS complexes, particularly in the limb leads. There may be a discrepancy of QRS voltages with signs of hypertrophy in V4-6 and relatively low voltages in the limb leads
- Abnormal Q waves are most often seen in leads V1 to V4 and may mimic the appearance of a myocardial infarction (“pseudoinfarction” pattern)
Dilated Cardiomyopathy Overview
Dilated cardiomyopathy (DCM) is a myocardial disease characterised by ventricular dilatation and global myocardial dysfunction (ejection fraction < 40%).
- Patients usually present with symptoms of biventricular failure, e.g. fatigue, dyspnoea, orthopnoea, ankle oedema
- Associated with a high mortality (2-year survival = 50%) due to progressive cardiogenic shock or ventricular dysrhythmias (sudden cardiac death)
Causes of Dilated Cardiomyopathy
Can be divided into ischaemic and non-ischaemic.
Ischaemic
- Dilated cardiomyopathy commonly occurs following massive anterior STEMI due to extensive myocardial necrosis and loss of contractility
Non-ischaemic
- Most cases are idiopathic
- Up to 25% are familial (primarily autosomal dominant, some types are X-linked)
A very small proportion may occur with:
- Viral myocarditis (coxsackie B / adenovirus)
- Alcoholism
- Toxins (e.g. doxorubicin)
- Autoimmune disease
- Pregnancy (peripartum cardiomyopathy)
ECG Examples
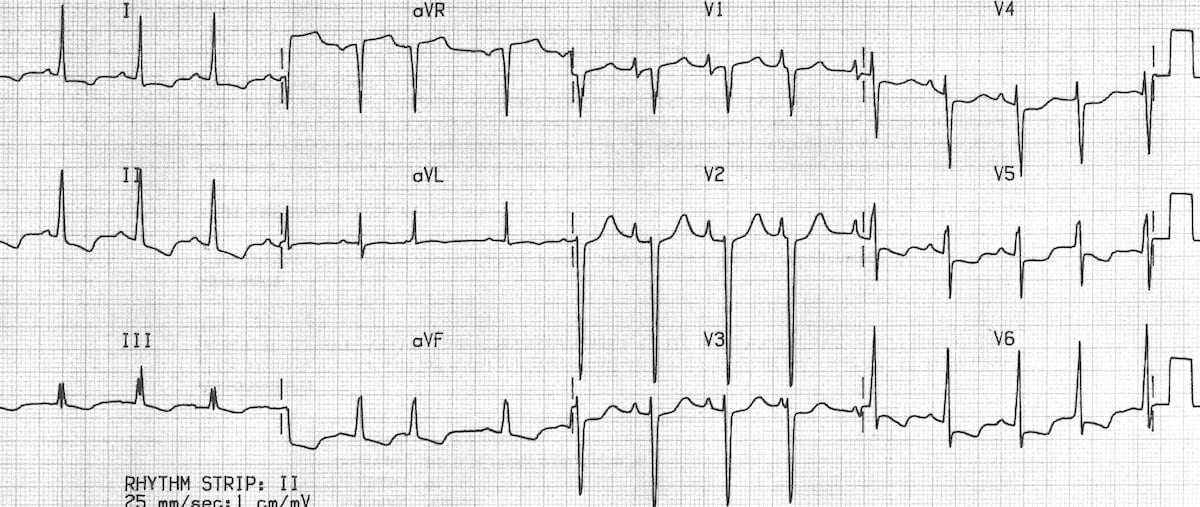
Example 1
Ischaemic cardiomyopathy:
- There is marked LVH (S wave in V2 > 35 mm) with dominant S waves in V1-4
- Right axis deviation suggests associated right ventricular hypertrophy (i.e. biventricular enlargement)
- There is evidence of left atrial enlargement (deep, wide terminal portion of the P wave in V1)
- There are peaked P waves in lead II suggestive of right atrial hypertrophy (not quite 2.5mm in height)
This patient had four-chamber dilatation on echocardiography with severe congestive cardiac failure (awaiting cardiac transplantation).
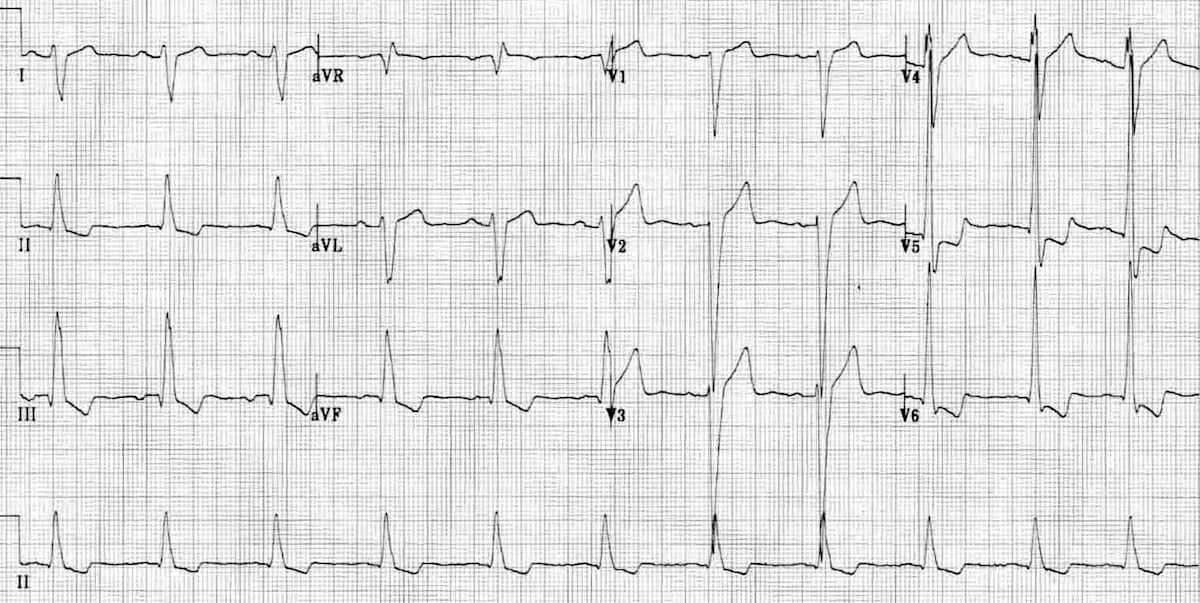
Example 2
Idiopathic dilated cardiomyopathy:
- There is evidence of left ventricular hypertrophy with large precordial voltages and an LV strain pattern in leads with a dominant R wave (I, II, V6)
- There is also evidence of biatrial enlargement in V1 with a peaked initial portion of the P wave (RAE) followed by a deep terminal negative portion (LAE)
- The changes of right ventricular hypertrophy are masked by left ventricular dominance; however, this patient had four-chamber dilatation on echocardiography
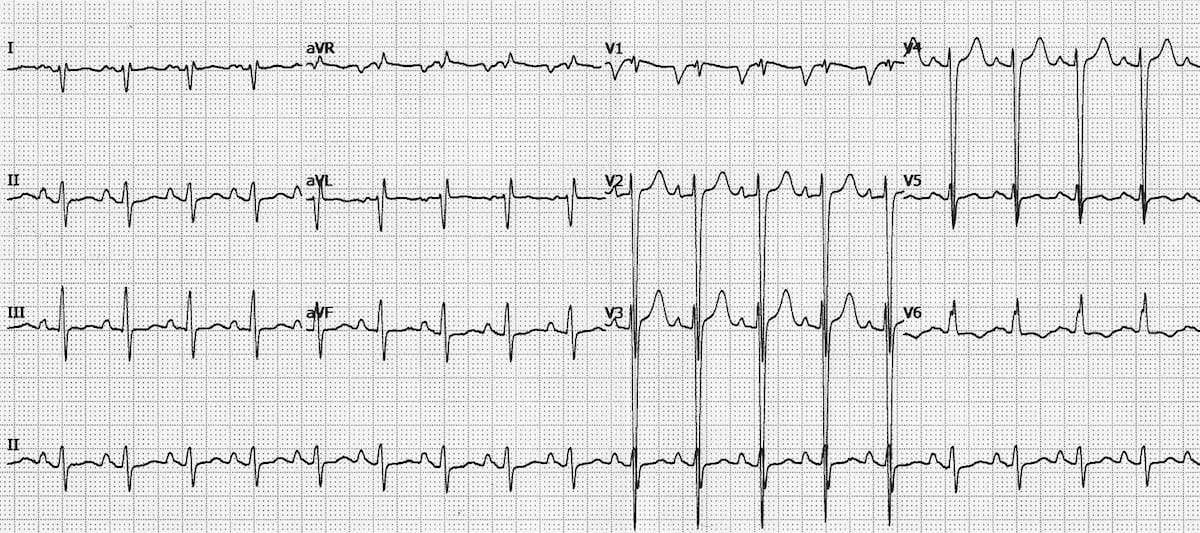
Example 3
Dilated cardiomyopathy:
- There is marked left ventricular hypertrophy with repolarisation abnormality (LV “strain” pattern) in V5-6
- LV dilatation has produced an interventricular conduction delay mimicking LBBB — however, this is not LBBB as the morphology is not typical and there are small Q waves in V5-6 (the presence of Q waves in V6 rules out LBBB)
- There are some signs of left atrial enlargement — leftward deviation of the P wave axis (positive P waves in I and aVL, inverted in III and aVF) and prolongation of the terminal portion of the P wave in V1
- Right axis deviation in the presence of LVH suggests the possibility of biventricular enlargement
- The widespread downsloping ST depression may be due to LVH (= “appropriate discordance”) or digoxin effect (a commonly used mediation in congestive cardiac failure)
Example 4

Dilated cardiomyopathy:
- Atrial fibrillation with LBBB is another ECG pattern commonly seen in DCM
Related Topics
References
- Edhouse J, Thakur RK, Khalil JM. ABC of clinical electrocardiography. Conditions affecting the left side of the heart. BMJ. 2002 May 25;324(7348):1264-7
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
ECG LIBRARY
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.