
![]()
ECG Case 113
65 year old male who was brought to the Emergency Department following an out-of-hospital cardiac arrest. ROSC was achieved prehospital following an episode of VT.
On arrival GCS 3, intubated with sats 98%, BP 75 systolic.
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
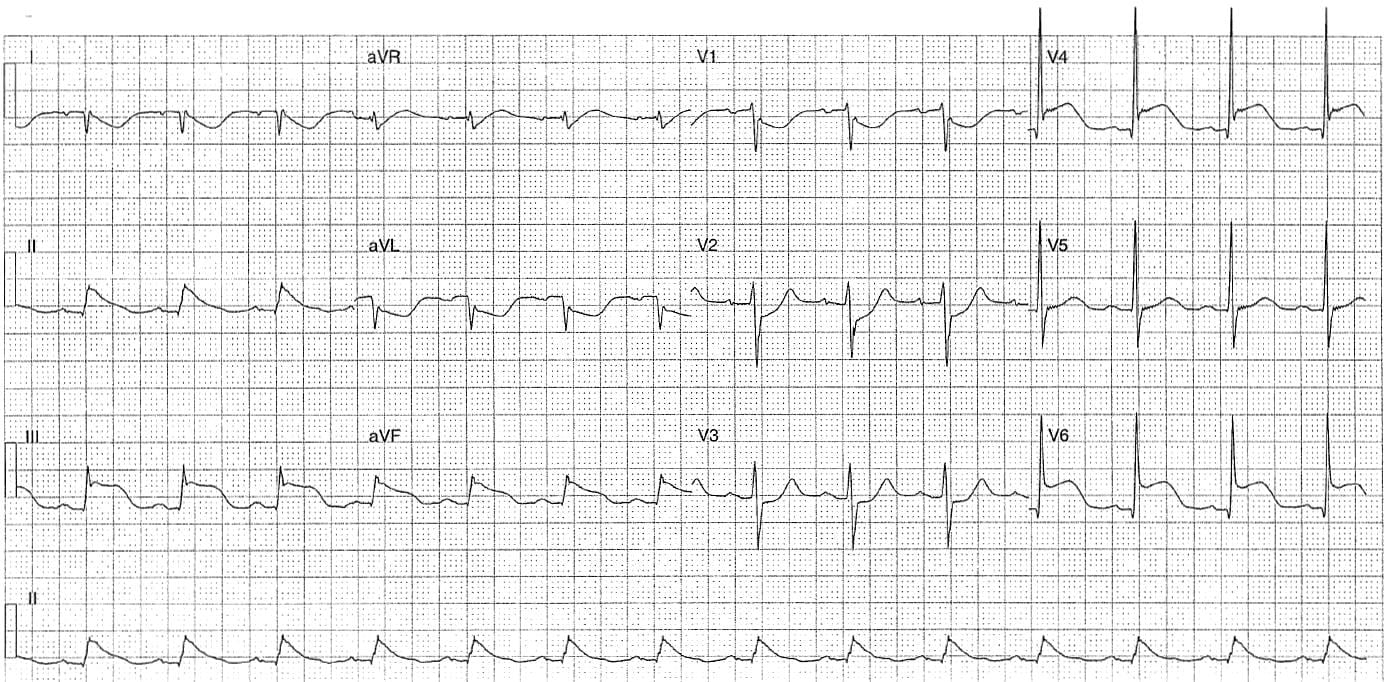
Rate:
- ~84 bpm
Rhythm:
- Regular
Axis:
- RAD
Intervals:
- PR – Prolonged(~220ms)
- QRS – Normal (80-100ms)
- QT – 400ms (QTc Bazette 470-480 ms)
Segments:
- ST Elevation leads II, III, aVF, V4, V6
- Unusual ST morphology in inferior leads
- ST depression lead aVL, V1-3
Additional:
- Note complete lead inversion leads I, aVL – negative P/QRS/T
Interpretation:
- STEMI
- Lead malposition
- Likely V4 & V5 reversed
- RA / LA limb lead reversal resultant inversion lead I, II/III switched and aVR/aVL switched
CLINICAL OUTCOME
What happened?
The patient was taken for urgent PCI which was normal!
He subsequently went on to have a CT brain which showed an extensive subarachnoid haemorrhage.
There are a number of cases in the literature where subarachnoid haemorrhage has been associated with significant ST changes:
- Van der Velden LBJ et al. Acute myocardial infarction complicating subarachnoid haemorrhage. Neth Heart J. 2009 Aug; 17(7-8): 284–287.
- I Beydilli et al. Subarachnoid Hemorrhage Mimicking Myocardial Infarction. The Internet Journal of Emergency Medicine. 2012; 7(2).
- S Chatterjeec. ECG Changes in Subarachnoid Haemorrhage: A Synopsis. Neth Heart J. 2011 Jan; 19(1): 31–34
Further Reading
- ECG Library – ECG Limb Lead Reversal
- ECG Library – ECG in Raised ICP
- ECG Library – STEMI – Posterior
- ECG Library – STEMI – Inferior
- ECG Library – STEMI – Lateral
TOP 150 ECG Series
Emergency Medicine Specialist MBChB FRCEM FACEM. Medical Education, Cardiology and Web Based Resources | @jjlarkin78 | LinkedIn |
