
![]()
ECG Case 133
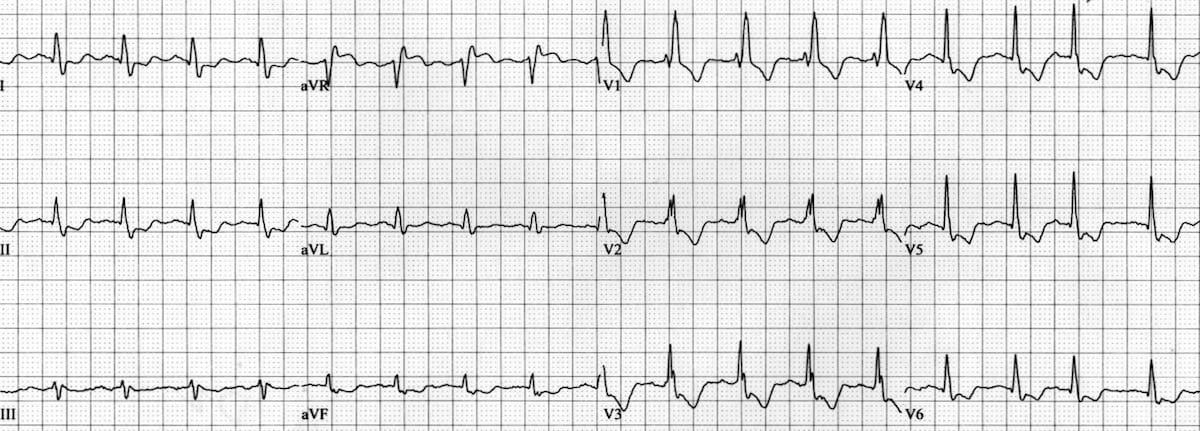
A 65-year-old woman presents with one hour of central chest pain following three days of exertional dyspnoea and lethargy. BP 79/51, HR 105 reg, SpO2 93 RA
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
- Normal sinus rhythm, rate 100 bpm
- Right bundle branch block
- Widespread ST depression, most notable in leads II and V4-6. Even in the context of RBBB, ST depression in V2-3 is excessively discordant
- ST elevation in aVR ~1mm
This ECG pattern simply represents diffuse subendocardial ischaemia due to oxygen supply-demand mismatch. It is the same ECG seen in patients that have a positive stress test. Note that ST elevation in aVR here is a reciprocal change to ST depression most marked in leads I, II and V4-6.
Some common clinical causes of this include:
- Hypotension or hypoxia
- Left main coronary artery (LMCA) or left anterior descending artery (LAD) stenosis/insufficiency
- Severe triple vessel disease
- ROSC post cardiac arrest
In the absence of ST elevation in other leads, acute coronary occlusion is rarely the cause of this ECG pattern.
ST elevation in aVR due to LMCA or “left main” occlusion is a misnomer — such a lesion causes simultaneous anterior, posterior and lateral STEMI leading to almost instantaneous death
OUTCOME
Initial work up in the emergency department revealed a Hb of 66, with malaena found on PR examination. The patient was resuscitated and transfused two units of packed cells, with resultant resolution of chest pain.
A repeat ECG taken following transfusion showed resolution of ST segment changes:

This patient likely has significant underlying ischaemic heart disease — either in the form of LMCA/LAD stenosis or triple vessel disease — which has been unmasked by haemodynamic compromise.
However, the LAST place they need to be during this acute illness is in the cath lab.
Delayed angiography would be appropriate to investigate coronary circulation but should not occur until the initial presentation has been resolved.
CLINICAL PEARLS
ST elevation in aVR: The failed stress test
The ECG pattern of widespread ST depression and reciprocal ST elevation in aVR simply represents subendocardial ischaemia. Although this is usually diffuse/global ischaemia, we must recall that ST depression of subendocardial ischaemia does not localise. It is the same ECG pattern seen in patients with a positive stress test.
When we see this pattern, we should think “oxygen supply-demand mismatch”. In patients that are shocked or post-arrest, be cautious in attributing these ECG changes solely to ACS. Although these patients may have a degree of underlying coronary artery disease making them more susceptible to this “ischaemic” pattern, haemodynamic compromise may be the underlying precipitant – as with our patient above, we must consider and address causes of this.
Almost any patient that has 20 minutes of no cardiac output will have a “positive” (failed) stress test. It does not necessarily mean they have an occluded coronary artery that requires reperfusion.
Take a look at this example. This ECG was taken 5 minutes post return of spontaneous circulation (ROSC) in a patient who suffered a VF arrest. He had known ischaemic heart disease:
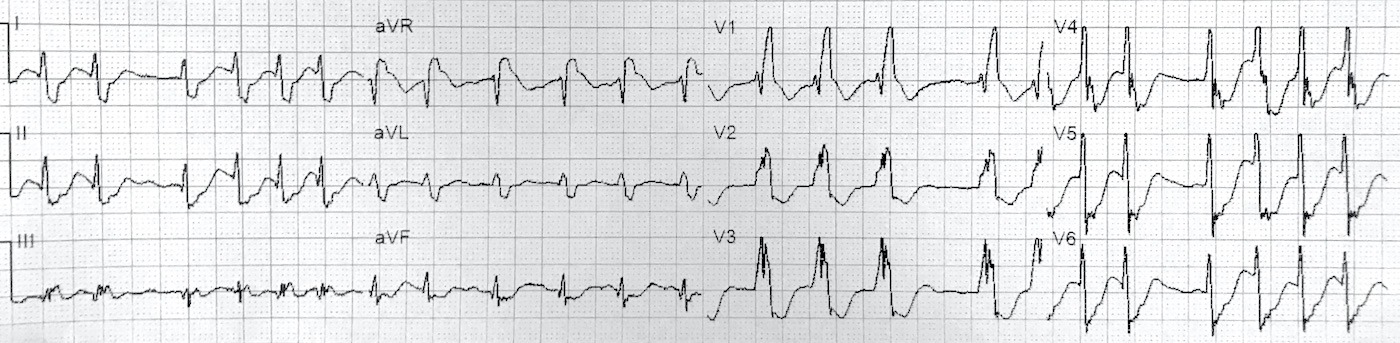
Note: ST depression in II and V4-6, with reciprocal ST elevation in aVR. Changes are significantly more pronounced than our patient with a GI bleed
At this stage, this ECG simply represents oxygen supply-demand mismatch, which is to be expected following extensive down time (20 minutes in this patient). This patient was taken for immediate angiography which demonstrated severe triple vessel disease but no acute occlusion.
In the absence of ST elevation in other leads, acute coronary occlusion is rarely the cause of this pattern
A 2019 single-centre retrospective analysis found that in patients undergoing code STEMI activations with this ECG pattern, only 59% had severe coronary artery disease, and only 10% had an occluded vessel (RCA or left circumflex artery). None had LMCA or LAD occlusions. 36% of these patients had presented in cardiac arrest.
In suspected ACS, ST elevation in aVR and diffuse ST depression warrants early discussion with cardiology and prompt (within 24-48 hours) angiography, but in the absence of ST elevation elsewhere, is usually not indicative of occlusion.
Which occlusion patterns can cause simultaneous ST elevation in aVR?
Lead aVR directly records electrical activity from the basal portion of the interventricular septum. Infarction to this area associated with proximal LAD occlusion can cause STE in aVR – however these patients will have associated features of anterior STEMI with ST elevation in V1-4.
Lastly, beware of Aslanger pattern, a specific ECG pattern representing acute inferior occlusion MI (OMI) in patients with concomitant multi-vessel disease The ST vector of subendocardial ischaemia directed towards aVR can mask inferior ST elevation, with resultant ST elevation only manifesting in lead III.
ST elevation in aVR due to LMCA or “left main” occlusion is a misnomer — such a lesion causes simultaneous anterior, posterior and lateral STEMI leading to almost instantaneous death
Immediate angiography is not always of benefit
Patients with severe myocardial ischaemia (from non-cardiac causes) may not only not benefit from coronary angiography, but may also receive harm. Injecting contrast into such a deranged circulation may result in abrupt haemodynamic deterioration.
The TOMAHAWK study published last month in NEJM compared immediate versus delayed angiography in patients successfully resuscitated following out-of-hospital cardiac arrest. All patients had no evidence of STEMI on post-resuscitation ECG. Immediate angiography provided no benefit over a delayed strategy with respect to the 30-day risk of death from any cause (54% mortality in immediate group versus 46% in delayed group).
- The pattern of diffuse ST depression (involving V4-6 and II) and ST elevation in aVR simply represents oxygen supply/demand mismatch — this can be a result of hypotension, hypoxia, or severe coronary artery disease
- In suspected ACS, ST elevation in aVR and diffuse ST depression warrants early discussion with cardiology and prompt (within 24-48 hours) angiography, but in the absence of ST elevation elsewhere, is usually not indicative of occlusion
- ST elevation in aVR due to LMCA or “left main” occlusion is a misnomer — such a lesion causes simultaneous anterior, posterior and lateral STEMI leading to almost instantaneous death
Further reading
Related topics
Expert Review
- Smith SW. Head On Motor Vehicle Collision. ST depression. Myocardial Contusion? Dr Smith’s ECG Blog. 2014 July
References
- Harhash et al. aVR ST Segment Elevation: Acute STEMI or Not? Incidence of an Acute Coronary Occlusion. Am J Med. 2019 May;132(5):622-630
- Desch et al. Angiography after Out-of-Hospital Cardiac Arrest without ST-Segment Elevation. NEJM. 2021 August. DOI: 10.1056/NEJMoa2101909
Further Reading
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
TOP 150 ECG Series

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.

Interventional cardiologist, ECG and hemodynamics fan. MD, Assoc. Prof. at Marmara University, Pendik T&R Hospital, Assoc. Editor at Archives of TSC, ESC National Prevention Coordinator
Great review. Thanks for all you do.
Sincerely,
A wandering paramedic
This website is really helpful for those who are interested in learning more about EKGs.
From an ER RN