
![]()
ECG Case 134
A 47-year-old woman presents with four hours of right shoulder pain and diaphoresis. HR 70 reg, BP 177/87, SpO2 95 RA.
An ECG is taken at triage.
The computer reads “inferior ischaemia” – do you agree?
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
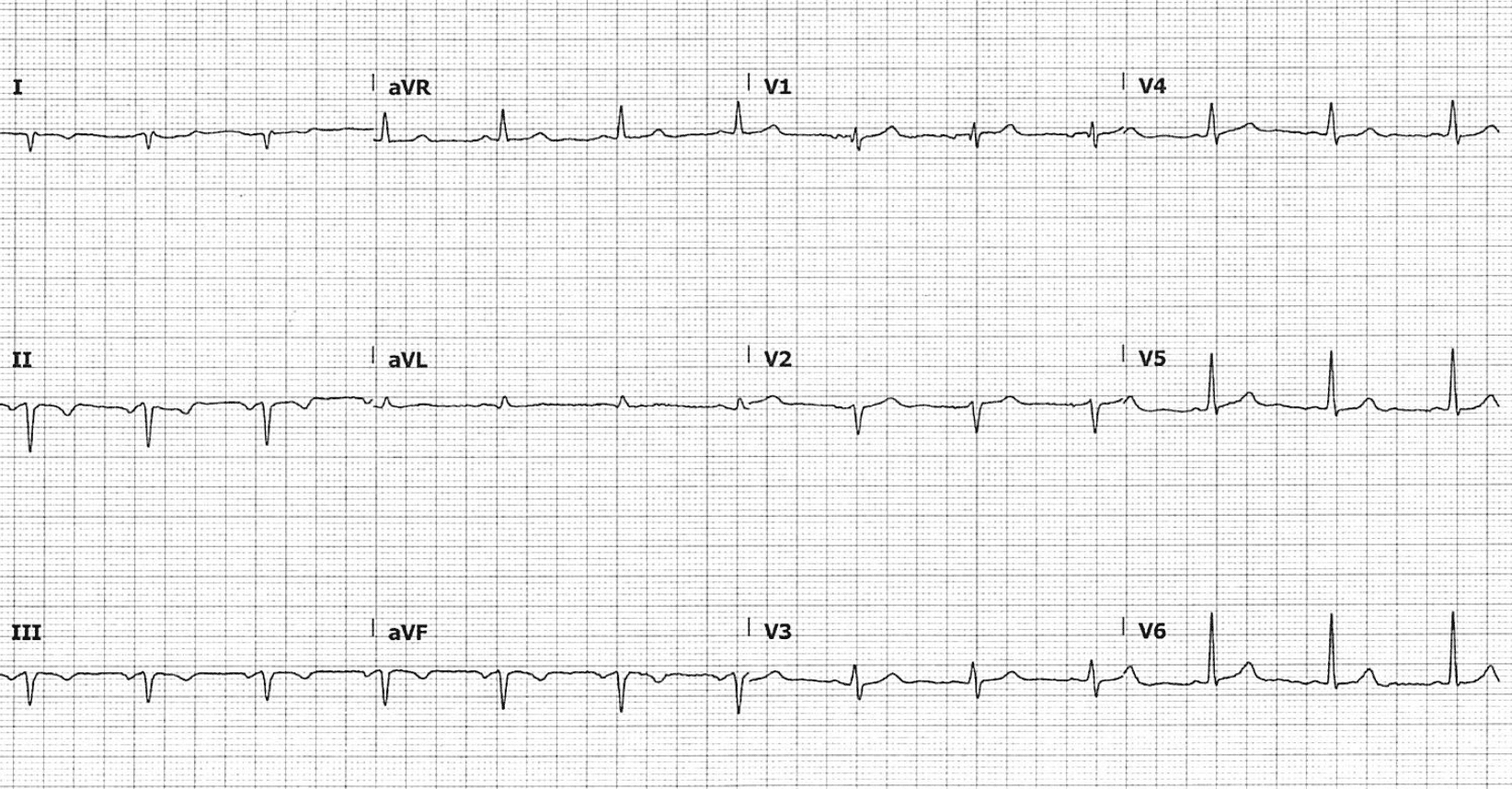
- Regular rhythm, rate 78 bpm
- P wave axis is abnormal – upright in aVR, negative in II – this is seen with ectopic atrial rhythms
- Northwest axis
- Q waves and T-wave inversion in leads I, II, III, aVF
- Precordial R wave progression is preserved
So, is this inferior ischaemia?
Reveal answer
No.
This is limb electrode misplacement leading to limb lead reversal. A northwest axis in an ECG with normal precordial leads simply does not make sense.
Although we assume correct lead placement when interpreting the ECG, an upright P-QRS-T complex in aVR with otherwise normal QRS conduction should raise suspicion for limb lead reversal.
OUTCOME
The ECG was repeated and positioning checked – indeed RA/LL electrodes were reversed. Repeat ECG demonstrated normal sinus rhythm with a normal QRS axis. This patient actually had acute cholecystitis and was admitted under the general surgical team.
CLINICAL PEARLS
System two thinking
Whilst some may immediately recognise the upright P-QRS-T wave complex in aVR as suspicious for limb lead reversal, many of us will be distracted by changes seen in inferior leads and the abnormal axis. This is where we need to go back to our system two approach — systematic, conscious, analytical interpretation of the ECG.
Our potential causes of a northwest axis include:
- Ventricular rhythms (ventricular tachycardia, accelerated idioventricular rhythm)
- Hyperkalaemia
- Extreme right axis deviation (RAD)
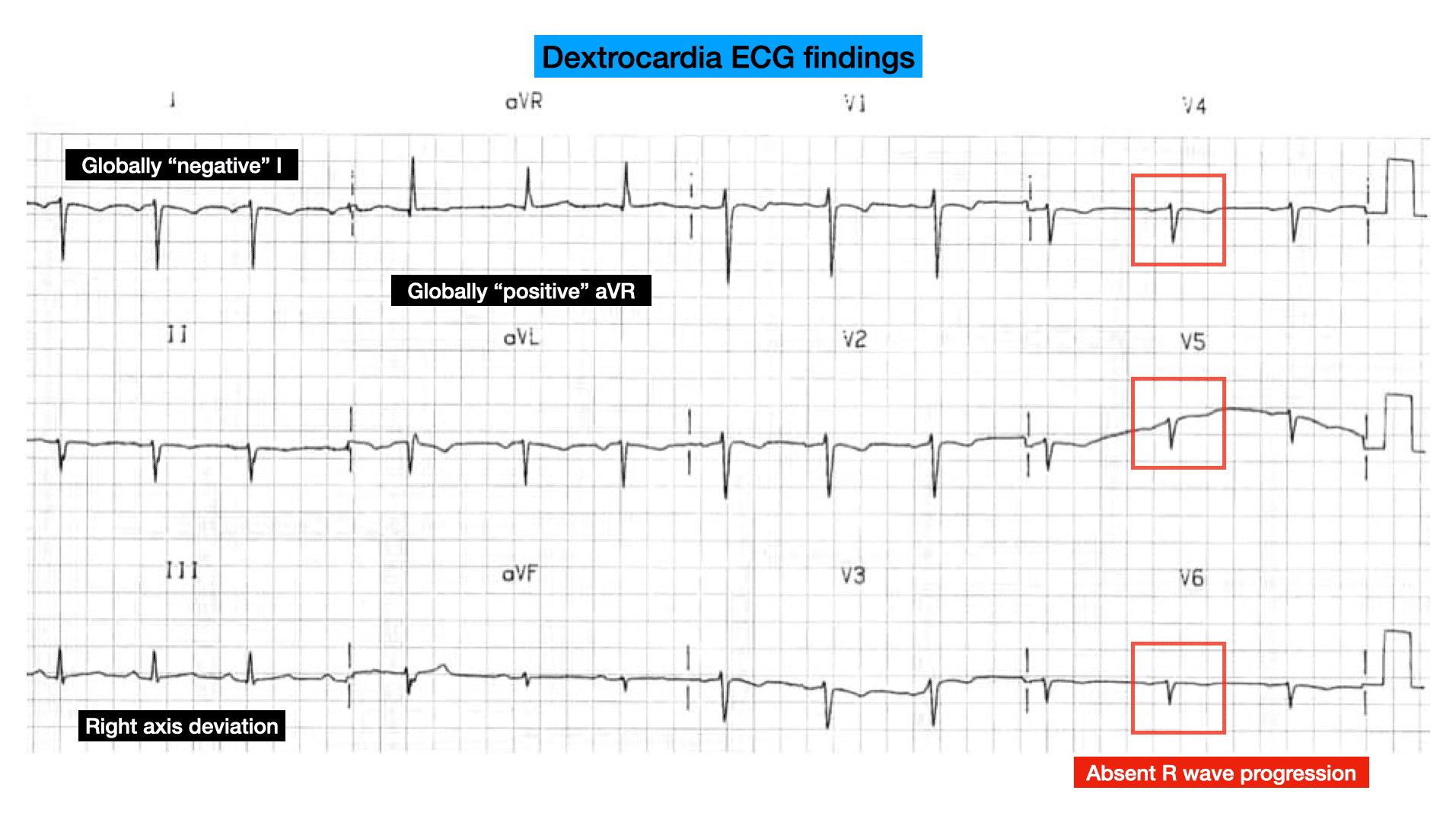
- Dextrocardia
A northwest axis in hyperkalaemia is a relatively late sign – we would expect significant intraventricular conduction delay and an abnormal QRS, often in the form of a sine wave appearance.
Extreme RAD is seen most often in the COPD patient with right ventricular strain and hyperinflated lungs causing a vertically orientated heart. We would see other associated features including a dominant R wave in V1 (suggestive of right ventricular hypertrophy), P pulmonale, and/or arrhythmias such as multifocal atrial tachycardia (MAT).
In dextrocardia, there is absent R wave progression in precordial leads – in fact, there is often R wave reversal as the lateral precordial leads move further away from the right-sided heart.
So where does this leave us? Well, a northwest axis in an ECG with normal precordial leads simply does not make sense. This must be lead misplacement.
Limb lead reversal
Limb lead electrode reversal is a common cause of ECG abnormality and may simulate ectopic atrial rhythm, chamber enlargement or ischaemia.
Recognising this pattern is easier if we understand the changes. Limb leads are calculated from left arm (LA), right arm (RA), and left leg (LL) electrodes.
For example, “lead I” = LA – RA, “lead II” = LL – RA, and so forth.
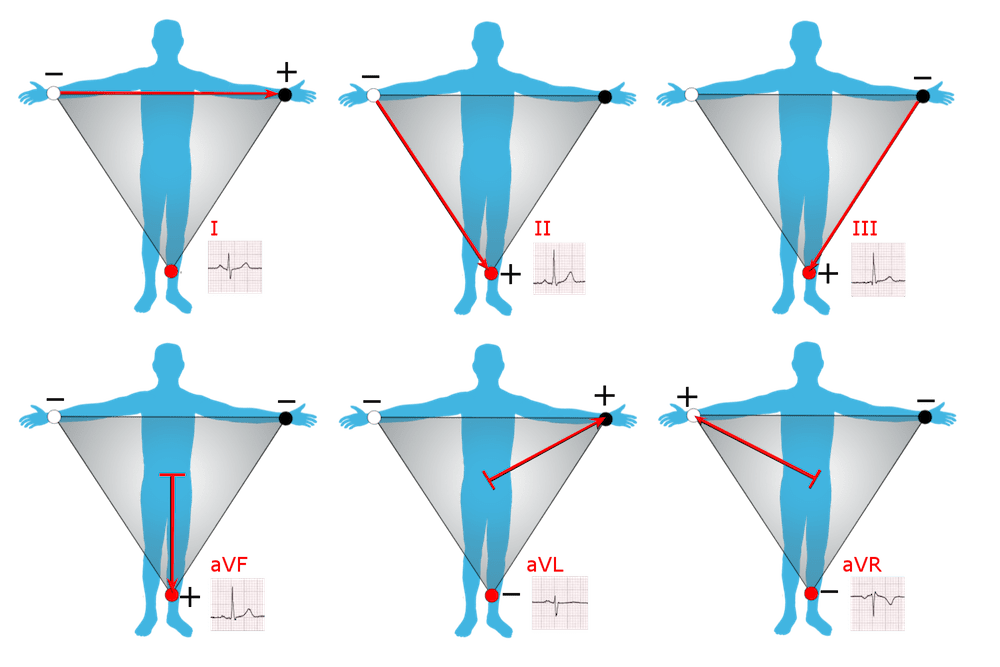
The above relationship between limb leads and electrodes can be described by Einthoven triangle:
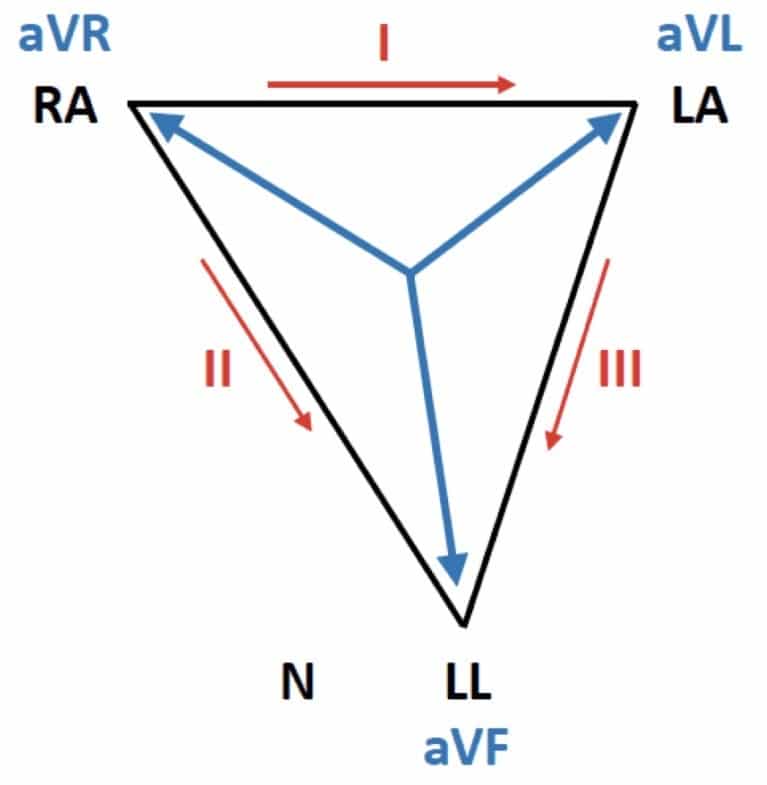
Our patient above has RA/LL electrode reversal. Their “triangle” has been flipped around the fixed LA vector. Most notably, aVF and aVR switch places. All of leads I, II and III are now “inverted”.
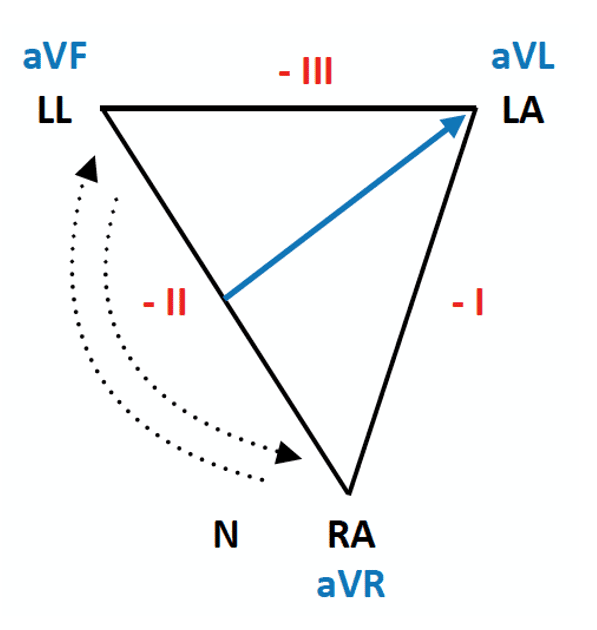
A quick guide to spotting RA/LL reversal:
- Lead aVR is uniformally upright
- Lead I, II, III and aVF are all completely inverted
It is a bit much, and not really necessary, to remember the exact changes in each type of limb lead reversal (there are multiple possibilities).
More relevant is that a uniformally positive P-QRS-T complex in aVR, or uniformally negative complex in lead I, should always prompt us to consider and check lead misplacement, especially when the QRS complex is otherwise normal.
You can read more about the different types of limb lead reversal here.
- Limb lead electrode reversal is a common cause of ECG abnormality and may simulate ectopic atrial rhythm, chamber enlargement or ischaemia
- In the absence of intraventricular conduction delay, a uniformally positive P-QRS-T complex in aVR or negative complex in I should prompt us to consider lead misplacement
- Preserved precordial R wave progression allows us to further differentiate from dextrocardia
Further reading
Related topics
Expert Review
- Smith SW. ST elevation in aVL with reciprocal ST depression in inferior leads and diffuse ST depression. Dr Smith’s ECG Blog. 2020 Feb
Further Reading
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
TOP 150 ECG Series

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.

Interventional cardiologist, ECG and hemodynamics fan. MD, Assoc. Prof. at Marmara University, Pendik T&R Hospital, Assoc. Editor at Archives of TSC, ESC National Prevention Coordinator
AVR is key to interpreting ekgs. Thanks.