
![]()
Lenègre-Lev disease
Acquired fibrous degeneration of the left and right bundle branches, eventually manifesting as permanent complete atrioventricular (AV) dissociation with cardiac pauses and Adams-Stokes attacks.
Also known as idiopathic fibrosis of the conducting system, or acquired complete heart block
Complete and permanent atrioventricular block is often the consequence of lesions involving both bundle branches, and not of a lesion in the common bundle
Ivan Mahaim: Les Maladies Organiques du Faisceau de His-Tawara. Paris, 1931
During his initial description, Lenègre consistently uses the term “Bilateral Bundle Branch Block” to describe this cardiac injury pattern that leads to AV dissociation. In 97% of cases the AV node is found to be histologically normal
Speed of progression to complete heart block is varied. Lenègre identified several ECG manifestations of bilateral bundle branch block:
- RBBB or LBBB complicated by complete or incomplete AV block
- Masqueraded Bundle Branch Block (MBBB)
- Complete heart block
The prognosis of Lenegre’s disease has been transformed by the development of electrical pacing.
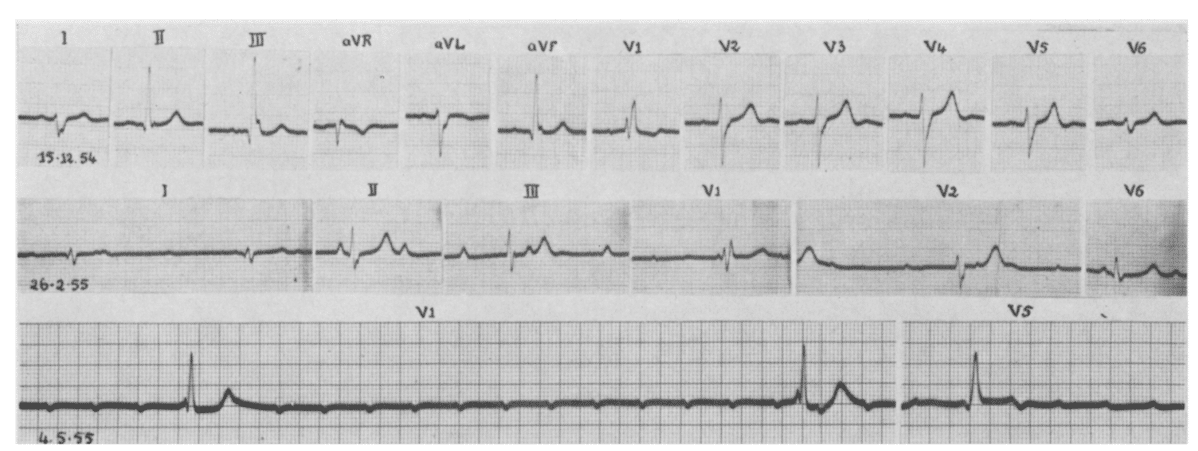
- ECG traces demonstrating progression of conducting system disease. Pathological specimens from the same patient showed extensive fibrous degeneration and replacement of the left and right bundle branches
- The first trace shows a complete RBBB with regular sinus rhythm, followed by a complete AV block with right ventricular delay, and finally a terminal extreme bradycardia
Disease associations
Although sometimes termed “idiopathic” fibrosis of the conducting system, degenerative changes seen are often a result of ischaemic heart disease, prior myocardial infarction, or long-standing hypertension and left ventricular hypertrophy
History of Lenègre-Lev disease
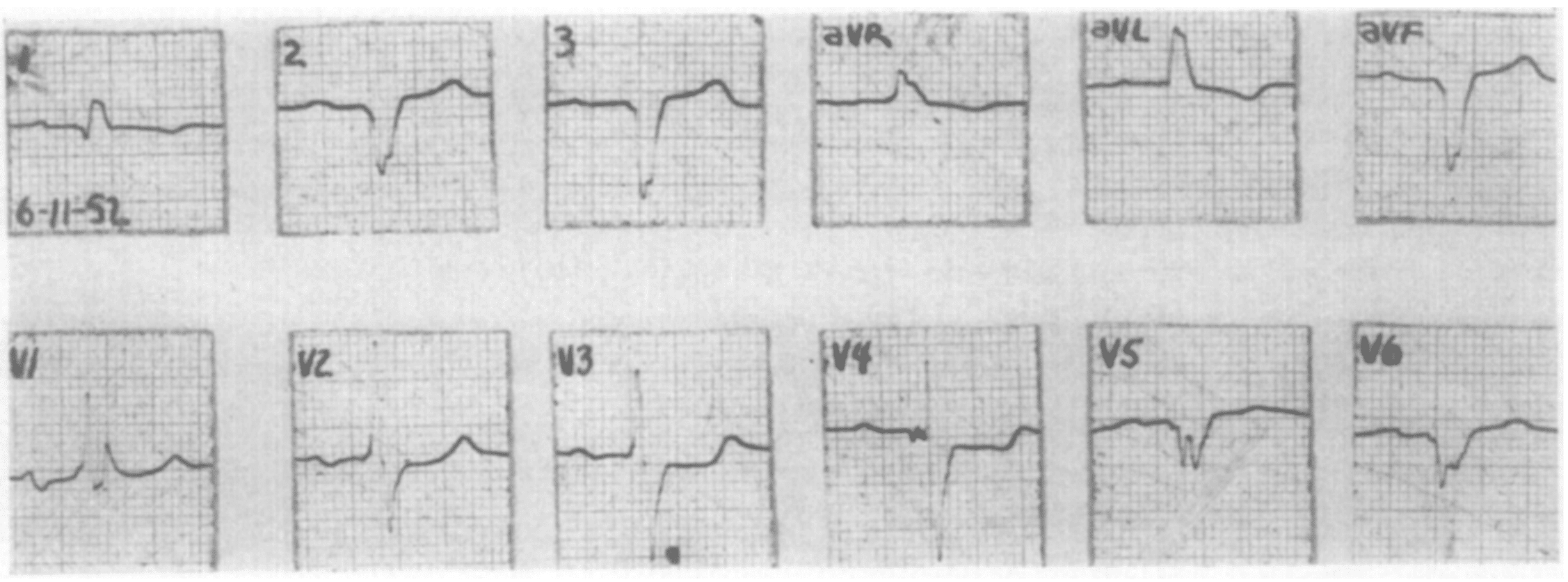
1954 – Richman and Wolff reported on “left bundle branch block masquerading as right bundle branch block” and described 4 cases which probably corresponded (especially case no. 1) to bilateral bundle branch block – a pattern of complete left bundle branch block in the standard leads and of complete right bundle branch block in the precordial leads.
1964 – Jean Lenègre, of the Hopital Boucicaut in Paris, described progressive fibrosis of the ventricular conduction system in a series of articles published in French in the 1950s:
Transformation fibreuse lente et progressive, d’origine dégénérative, des deux branches du faisceau de His, entraînant des troubles conductionnels progressifs : bloc de branche avec ou sans hémibloc du côté opposé, puis bloc auriculoventriculaire complet, paroxystique puis permanent (maladie d’Adams-Stokes)
His first and major reference in English appeared in 1964 as “Etiology and pathology of bilateral bundle branch block in relation to complete heart block“
1964 – Maurice Lev, of the University of Miami, saw a similar sclerodegenerative process, often with calcification, in an older age group publishing “Anatomic basis for atrioventricular block“
Both processes are manifested as fascicular conduction defects shown in the electrocardiogram, somewhat more rapidly progressing toward complete atrioventricular block in Lenegre’s disease than in Lev’s
Semantically, both are diseases – as originally proposed by Rosenbaum (1970) – rather than syndromes: Each consists of an essentially monocomponent pathology.
Associated Persons
- Jean Lenègre (1904-1972)
- Maurice Lev (1908-1994)
Alternate names
- Lev’s disease
- Lenègre’s disease
- Maladie de Lenègre (fibrose des deux branches du faisceau de His à l’origine de troubles progressifs de la conduction)
Controversies
Described independently by Jean Lenègre and Maurice Lev in 1964. Generally referred to as Lev’s disease. However, Lenègre published (in French) the condition 10 years earlier.
To the editor: Perhaps I may be able to help Dr. Perry with the following points on the Lev and Lenègre “syndromes.” Jean Lenègre, of the Hôpital Boucicaut in Paris, described progressive fibrosis of the ventricular conduction system in a series of articles published in French in the 1950s; his first and major reference in English appeared in 1964.
Maurice Lev, of the University of Miami, saw a similar sclerodegenerative process, often with calcification, in an older age group. Both processes are manifested as fascicular conduction defects shown in the electrocardiogram, somewhat more rapidly progressing toward complete atrioventricular block in Lenègre disease rather than Lev’s. The clinical recognition of these diseases requires exclusion of other forms of heart disease.
Semantically both are diseases – as originally proposed by Rosenbaum – rather than syndromes: Each consists of an essentially monocomponent pathology. Confusion notwithstanding Lenègre’s name could have been retained in its original form
George Nikolic 1983
References
Historical articles
- Mahaim I. Les maladies organiques de faisceau de His-Tawara les syndromes coronaires. – L’endocardite septale. – L’infarctus septal. (Etude clinique et anatomique). 1931
- Yater WM, Cornell VH, Claytor T. Auriculoventricular heart block due to bilateral bundle-branch lesions; review of the literature and report of three cases with detailed histopathologic studies. Arch Intern Med (Chic). 1936;57(1):132-173
- Richman JL, Wolff L. Left bundle branch block masquerading as right bundle branch block. Am Heart J. 1954; 47(3): 383-393.
- Lenègre J. Etiology and pathology of bilateral bundle branch block in relation to complete heart block. Prog Cardiovasc Dis 1964; 6: 409-444
- Lev M. Anatomic basis for atrioventricular block. Am J Med 1964; 37: 742-8.
Review articles
- Rosenbaum MB. The hemiblocks: diagnostic criteria and clinical significance. Mod Concepts Cardiovasc Dis. 1970; 39(12): 141-146
- Perry RJ. The Lev and LeNegre Syndromes. Annals of Internal Medicine, 1982; 97(6): 932
- Nikolic G. Lev and Lenègre Diseases. Annals of Internal Medicine, 1983; 98(3): 414
eponymictionary
the names behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.