
![]()
AV block: 3rd degree (complete heart block)
ECG features of complete heart block
- Severe bradycardia due to absence of AV conduction
- The ECG demonstrates complete AV dissociation, with independent atrial and ventricular rates
In complete heart block, there is complete absence of AV conduction, with none of the supraventricular impulses conducted to the ventricles. The perfusing rhythm is maintained by junctional or ventricular escape rhythm. Alternatively, the patient may suffer ventricular standstill leading to syncope (if self-terminating) or sudden cardiac death (if prolonged).
Pathophysiology
- Complete heart block is essentially the end point of either Mobitz I or Mobitz II AV block
- It may be due to progressive fatigue of AV nodal cells as per Mobitz I (e.g. secondary to increased vagal tone in the acute phase of an inferior MI)
- Alternatively, it may be due to sudden onset of complete conduction failure throughout the His-Purkinje system, as per Mobitz II. This can be secondary to septal infarction in acute anterior MI, or as a result of progression of conducting system disease causing true trifascicular block
- The former is more likely to respond to atropine and has a better overall prognosis
Causes of complete heart block
The causes are the same as for Mobitz I and Mobitz II second degree heart block. The most important aetiologies are:
- Inferior myocardial infarction
- AV-nodal blocking drugs (e.g. calcium-channel blockers, beta-blockers, digoxin)
- Idiopathic degeneration of the conducting system (Lenegre’s or Lev’s disease), causing true trifascicular block
Clinical significance
- Patients with third degree heart block are at high risk of ventricular standstill and sudden cardiac death
- They require urgent admission for cardiac monitoring, backup temporary pacing and usually insertion of a permanent pacemaker
Differential diagnosis
Complete heart block should not be confused with:
- High grade AV block: A type of severe second degree heart block with a very slow ventricular rate but still some evidence of occasional AV conduction
- AV dissociation: This term indicates only the occurrence of independent atrial and ventricular contractions and may be caused by entities other than complete heart block (e.g. “interference-dissociation” due to the presence of a ventricular rhythm such as AIVR or VT)
ECG Examples
Example 1
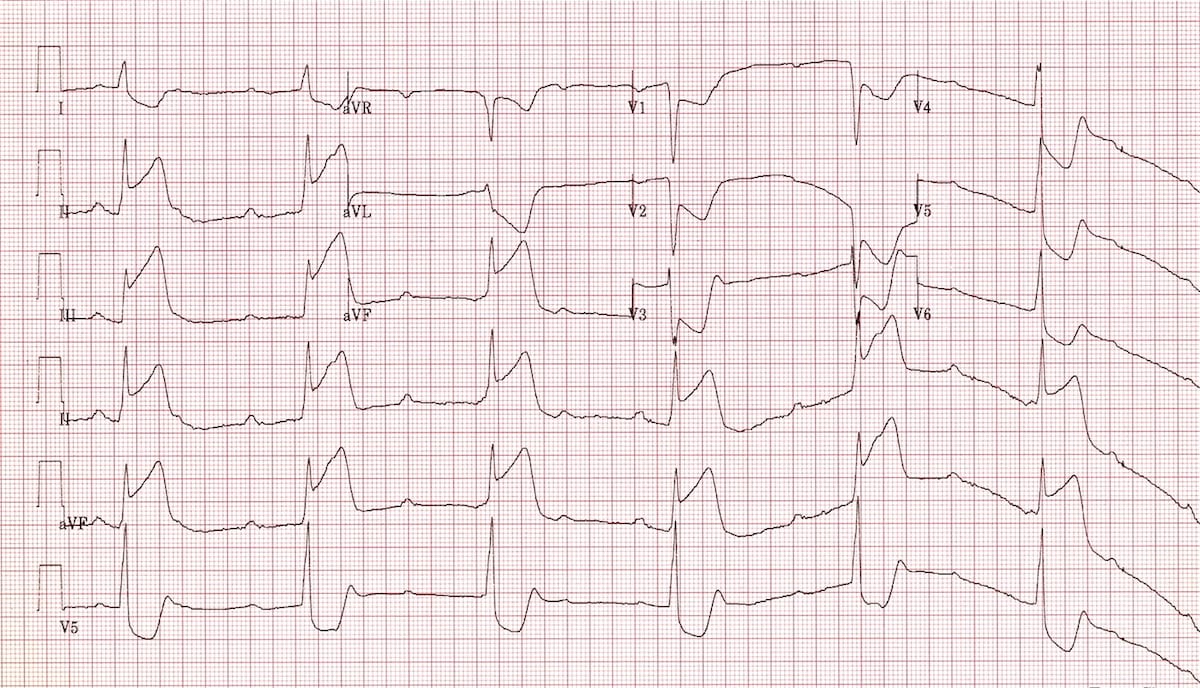
Complete Heart Block:
- Atrial rate is ~ 85 bpm
- Ventricular rate is ~ 38 bpm
- None of the atrial impulses appear to be conducted to the ventricles
- Rhythm is maintained by a junctional escape rhythm
- Marked inferior ST elevation indicates that the cause is an inferior STEMI
Example 2

Complete Heart Block:
- Atrial rate is ~ 60 bpm
- Ventricular rate is ~ 27 bpm
- None of the atrial impulses appear to be conducted to the ventricles
- There is a slow ventricular escape rhythm
Example 3
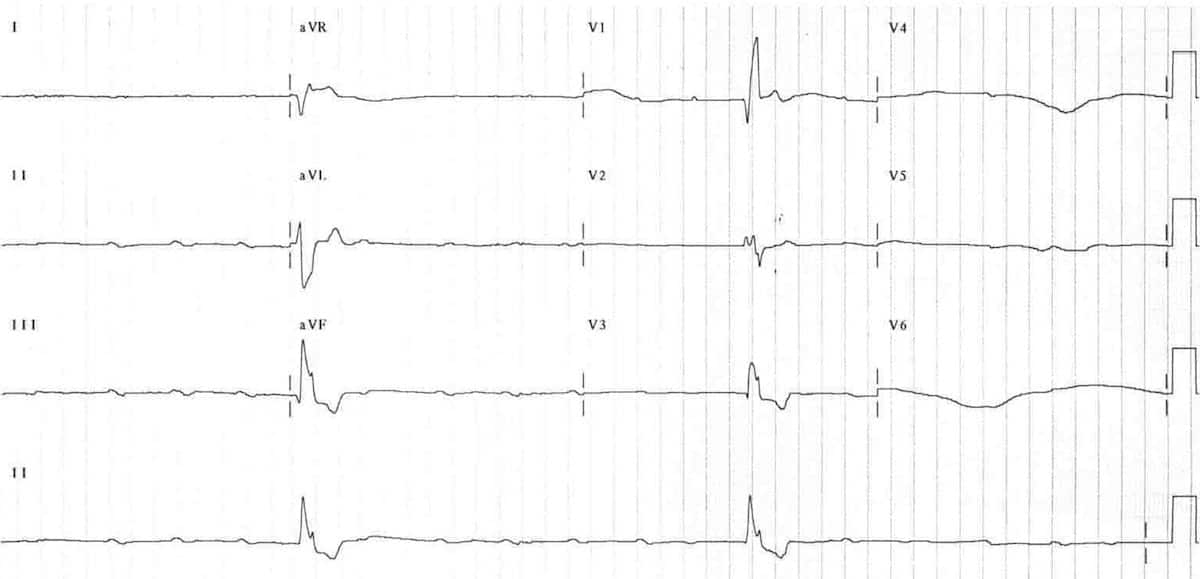
Complete Heart Block:
- Atrial rate 100 bpm
- Ventricular rate only 15 bpm!
- This patient needs urgent treatment with atropine / isoprenaline and pacing!
Example 4

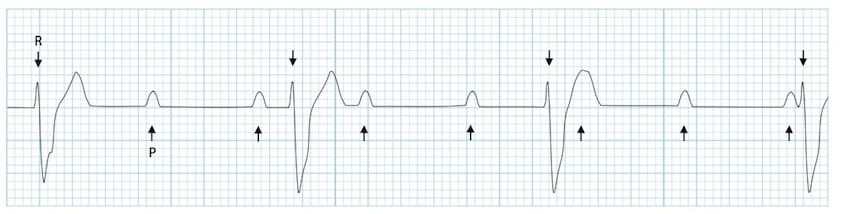
Complete Heart Block with Isorhythmic AV Dissociation (long rhythm strip):
- Atrial rate ~ 85 bpm
- Ventricular rate ~ 42bpm
- There is a junctional escape rhythm
- As the ventricular rate is approximately half the atrial rate, this rhythm at first glance appears to be second-degree AV block with 2:1 conduction
- However, on closer inspection, the PR interval varies with some of the P waves superimposed on the QRS complexes. The ventricular rate remains regular
- This confirms that the atrial impulses are not being conducted to the ventricles
- The apparent relationship between the P waves and QRS complexes occurs merely by chance (= isorhythmic AV dissociation)
Related Topics
- AV block: 1st degree
- AV block: 2nd degree, Mobitz I
- AV block: 2nd degree, Mobitz II
- AV block: 2nd degree, “fixed ratio blocks” (2:1, 3:1)
- AV block: 2nd degree, “high grade AV block”
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
ECG LIBRARY
Emergency Medicine Specialist MBChB FRCEM FACEM. Medical Education, Cardiology and Web Based Resources | @jjlarkin78 | LinkedIn |

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.
Hi John, thanks for the great article. Just double checking on example 3 with the wide-complex bradyarrhythmia, I’m a bit confused about when we use atropine and when this might not be effective if the level of the block is below the AV node. Does the wide-complex escape rhythm always indicate the block is below the AV node? If so, does that mean that the atropine might not be effective, or, if the BP is very low is it still worth trying the atropine? Cheers, thanks again, Annie
Ps is there any way we can tell if the block is at the level of the Bundle of His rather than the AV node? Pps, do you ever use adrenaline instead of isoprenaline if the BP is very low?
(The two rates are independent; there is no evidence that any of the atrial impulses are conducted to the ventricles.) what could be the evidence ?
Great content as always. Just echoing Annie’s comment, having had a case of complete HB that was unresponsive to atropine and then carrying out further research I’m led to believe that its incredibly rare that 3rd degree is responsive to atropine.