
![]()
Samuel A. Levine
Samuel Albert Levine (1891-1966) Polish-American cardiologist
Innovator in the treatment of coronary thrombosis patients. He recommended arm-chair recuperation within the first few days following an attack, instead of traditional bed rest.
An early advocate for the use of the ‘mechanical-electro-cardiograph’ to study heart patients, but he impressed upon his students the value of simple bedside methods of examination. He believed a physician should use the cardiogram to supplement his stethoscope.
Levine published over 250 articles; contributed to the pathophysiology understanding of pernicious anaemia (the lack of gastric hydrochloric acid); and reported one of the first successful cases of mitral valvulotomy in a 12-year-old girl.
Eponymously remembered for Levine Grading Scale (1933); Lown–Ganong–Levine syndrome (1952); the Levine sign; and Samuel A. Levine Professorship [Harvard, 1954 founded with a gift from the late Charles E. Merrill of New York]
Biography
- Born on January 1, 1891 in Łomża, Poland
- 1894 – Relocated to Boston, USA, aged 3
- 1914 – Graduated from Harvard Medical School. Undertook internship at the Peter Bent Brigham Hospital, and a fellowship at the Rockefeller Institute.
- 1917 – Volunteered to join the British medical corps during World War 1. Levine was assigned to the British Heart Hospital, Colchester, where he worked under renowned cardiologists: Sir Clifford Allbutt, Sir William Osler, Sir James McKenzie, and Sir Thomas Lewis.
- 1919 – Returned to the Peter Bent Brigham Hospital
- 1921 – Advised the diagnosis of poliomyelitis for the paralytic illness of future President Franklin D. Roosevelt.
- 1921 – Started a summer postgraduate cardiology course, which ran for 36 years at Harvard Medical School – the longest running course at the University.
- 1940 – Appointed physician at Peter Bent Brigham Hospital
- 1948 – Clinical Professor of Medicine at Harvard
- Died March 31, 1966, in Massachusetts
Medical Eponyms
Lown–Ganong–Levine syndrome (1952)
Proposed pre-excitation syndrome. Accessory pathway composed of James fibres. Characteristic ECG findings of short PR interval (<120ms); normal P wave axis; normal/narrow QRS morphology in the presence of paroxysmal tachycardia. [Lown B – Ganong WF – Levine SA]
Existence of LGL is disputed and the condition may not actually exist…the term should not be used in the absence of paroxysmal tachycardia
Levine Scale (Levine Grading Scale) (1933)
Six-point grading system that is used to define the volume or intensity of a heart murmur with an acoustic stethoscope. Levine addressed the clinical significance of the systolic murmur in two publications in 1933.
…for some years I have expressed the intensity of the systolic murmur in six gradations. Grade 1 is the faintest bruit that can be heard on careful auscultation. Although faint, it must have a definite duration into systole. This can be called a slightest possible murmur. Such murmurs are frequently overlooked in general practice.
A murmur of grade 6 intensity is extremely rare and may be applied to the few instances in which the murmur can be heard with the naked ear held even at some distance from the chest wall. This one may be called the loudest possible murmur.
Murmurs of grades 2 to 5 are intermediate and may be designated slight murmur, moderate murmur, loud murmur, and very loud murmur. It is remarkable that with a very little experience independent observers will designate the same murmur with practically identical terms.
Physicians who have worked with me for a short time will differ by no more than one gradation, and in the majority of instances there has been absolute agreement. This has been gone into in some detail because I believe that without such a nomenclature there will be only confusion and no progress in the clinical interpretation of systolic murmurs.
Levine 1933
- Grade 1: Faint. Heard only after a few seconds have elapsed
- Grade 2: A faint murmur heard immediately
- Grade 3: Moderately loud murmur
- Grade 4: Loud murmur
- Grade 5: Very loud murmur. Can be heard if only the edge of the stethoscope is in contact with the skin.
- Grade 6: Loudest possible murmur. The murmur can be heard with the stethoscope just removed from the chest and not touching the skin.
Levine’s system is often misused. For example, a soft murmur heard immediately is often labeled grade 1 instead of grade 2, as specified in the Levine classification. Furthermore, a grade 4 murmur on the Levine grading scale does not require the presence of a thrill, as is commonly taught. [Silverman 2008]
Levine sign
In 1934, the Argentinian cardiologist Pedro Cossio (1900-1986) described the ‘Palm sign’ – extended palm placed against the sternum to define ischaemic chest pain (67% sensitive; 38% specific). This is referred to as the Cossio-Levine Sign
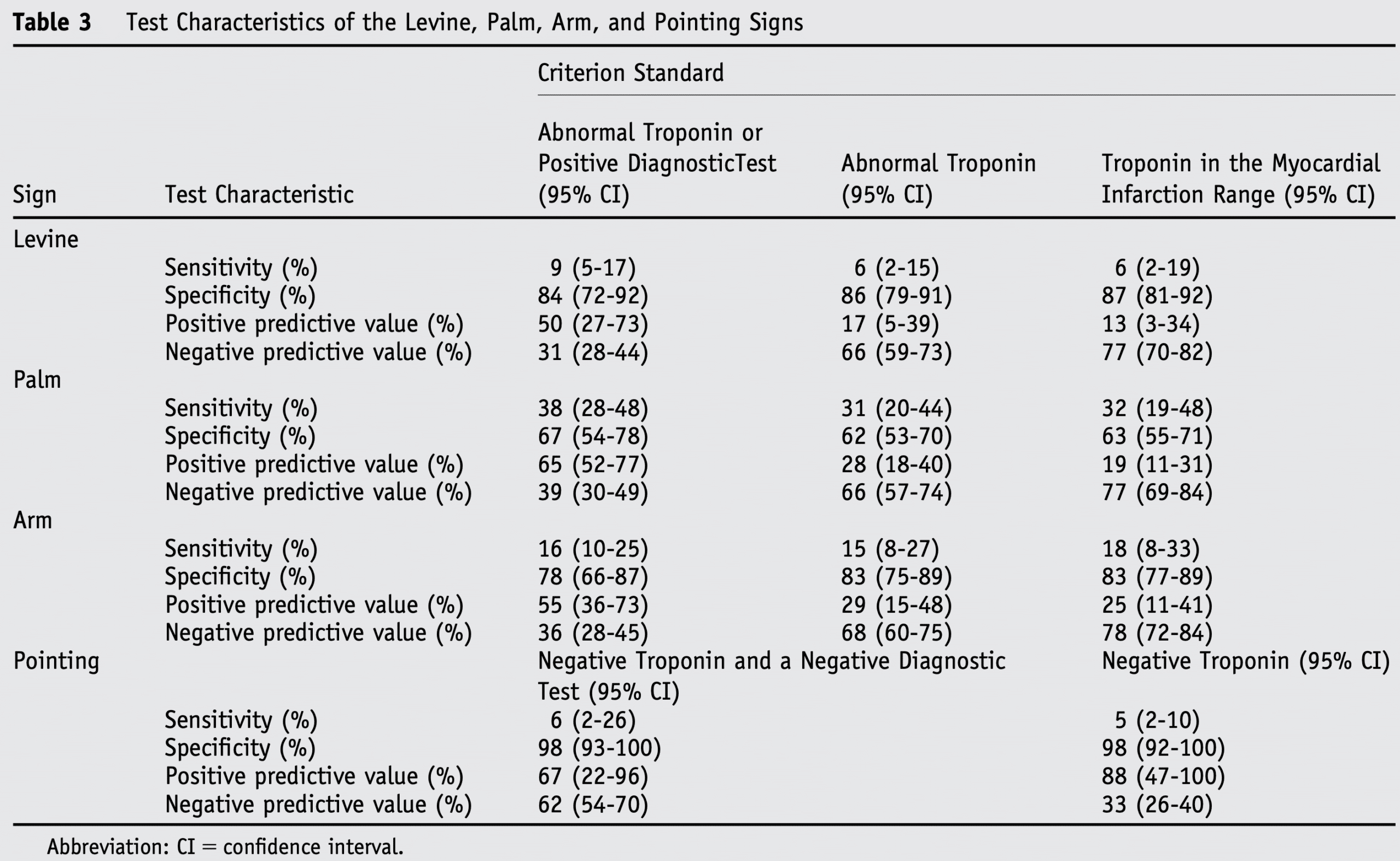
Levine taught that a ‘clenching the fist over the chest whilst describing pain increased the potential that the pain was ischaemic in nature‘ (84% specific but 9% sensitive for ischaemic heart disease; Table 3). No specific published work by Levine SA, but referenced in major cardiology textbooks to acknowledge the bedside teachings of Levine. Original source of term still being sought.
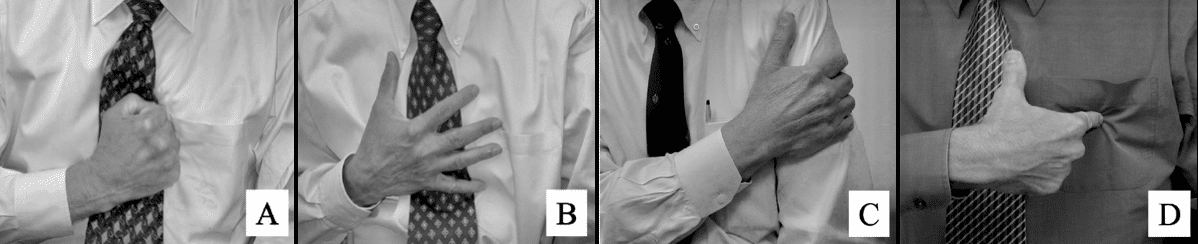
(A) Levine Sign. (B) Palm Sign. (C) Arm Sign. (D) Pointing Sign. Marcus et al 2007
Marcus et al examined gestures exhibited by patients admitted with chest discomfort as described in the medical literature. They concluded that contrary to traditional clinical teaching, direct examination of these gestures fails to demonstrate clinical utility. However, the clinical value of the gestures may be related to a communication of the size of the chest discomfort, with larger diameters more indicative of cardiac ischaemia.
Controversies
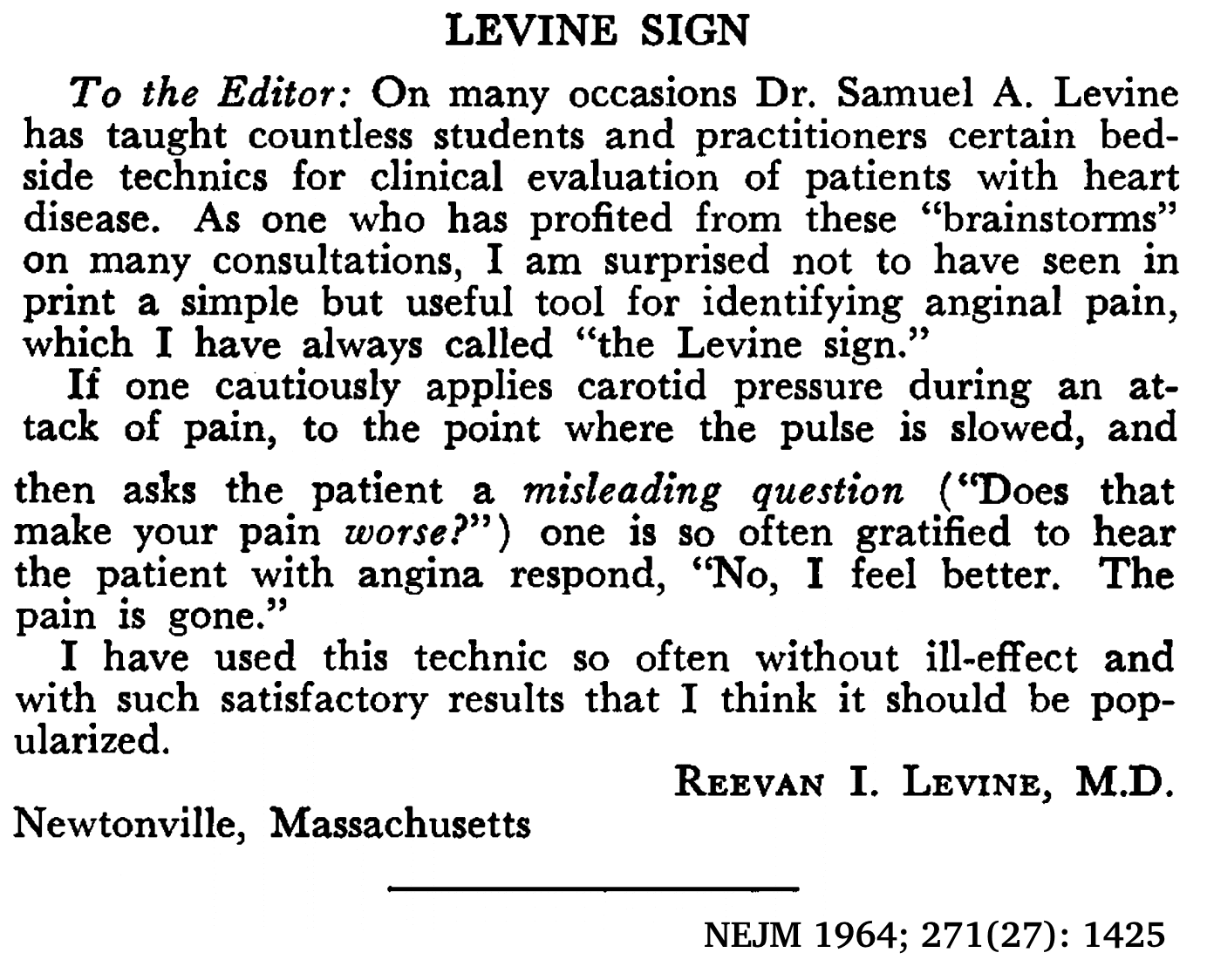
Levine sign II
Of note, Levine RI wrote to the NEJM to have a alternate ‘Levine sign‘ popularised – that is, the use of carotid massage to slow the pulse in patients presenting with chest pain, with an easing of the pain ‘confirming’ the an ischaemic in origin…
Major Publications
- Levine SA, Tranter CL. Infarction of the heart simulating acute surgical abdominal conditions. American Journal Of The Medical Sciences. 1918;155:57-65.
- Levine SA, Ladd WS. Pernicious anemia: A clinical study of one hundred and fifty consecutive cases with special reference to gastric anacidity. Johns Hopkins Hospital Bulletin. 1921;32(366):254-286.
- Cutler EC, Levine SA: Cardiotomy and valvulotomy for mitral stenosis: Experimental observations and clinical notes concerning an operated case with recovery. Boston Medical and Surgical Journal. 1923;188:1023-27
- Levine SA. Coronary Thrombosis: Its Various Clinical Features. Medicine 1929; 8: 245-418 [Dressler syndrome]
- Levine SA. The systolic murmur: its clinical significance. JAMA 1933; 101(6): 436–438. [Levine Grading Scale for cardiac murmurs]
- Freeman AR, Levine SA. The clinical significance of the systolic murmur. A study of 1000 consecutive “non-cardiac” cases. Ann Intern Med 1933; 6: 1371-1385. [Levine Grading Scale]
- Levine S, Harvey W. Clinical auscultation of the heart. Philadelphia: WB Saunders, 1949. [‘The Little Green Book‘]
- Levine SA. Clinical Heart Disease. 1936.
- Levine SA, Lown B. The “chair” treatment of acute thrombosis. Trans Assoc Am Physicians. 1951;64:316-27.
Levine SA, Lown B. “Armchair” treatment of acute coronary thrombosis. J Am Med Assoc. 1952 Apr 19;148(16):1365-9 - Lown B, Ganong WF, Levine SA. The syndrome of short P-R interval, normal QRS complex and paroxysmal rapid heart action. Circulation. 1952 May;5(5):693-706 [Lown–Ganong–Levine syndrome]
References
Biography
- Samuel Albert Levine (1891-1966). Br Heart J. 1966;28(6):853-4
- Levine HJ. Samuel A. Levine (1891-1966). Clin Cardiol. 1992 Jun;15(6):473-6
- Bibliography. Levine, Samuel A. WorldCat Identities
Eponymous terms
- Levine RI. Levine Sign. New England Journal of Medicine, 1964; 271(27): 1425–1425.
- Edmondstone WM. Cardiac chest pain: does body language help the diagnosis? 1995; BMJ. 311 (7021): 1660–1
- Marcus GM et al. The utility of gestures in patients with chest discomfort. Am J Med. 2007; 120(1): 83-89.
- Silverman ME, Wooley CF. Samuel A. Levine and the history of grading systolic murmurs. Am J Cardiol. 2008; 102(8): 1107-1110
- Long N. Funtabulously Frivolous Friday Five 277. LITFL
Eponym
the person behind the name
Doctor in Australia. Keen interest in internal medicine, medical education, and medical history.
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |