
![]()
Lown–Ganong–Levine syndrome
Description
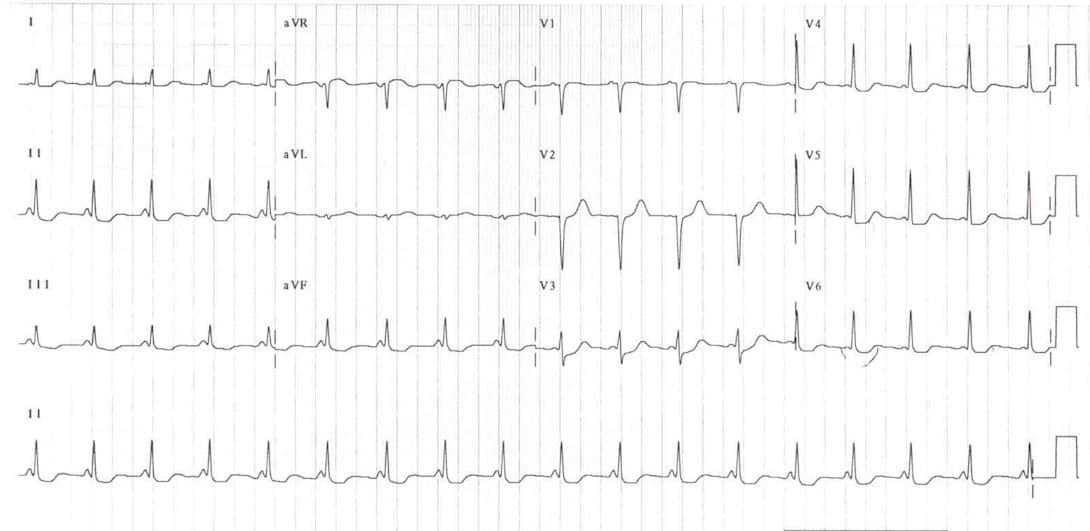
Lown–Ganong–Levine syndrome (LGL): Proposed pre-excitation syndrome. Accessory pathway composed of James fibres. Characteristic ECG findings of short PR interval (<120ms); normal P wave axis; normal/narrow QRS morphology in the presence of paroxysmal tachyarrhythmia.
Existence of LGL is disputed and the condition may not actually exist…the term should not be used in the absence of paroxysmal tachycardia
History of Lown–Ganong–Levine syndrome
1921-1952 association of paroxysmal tachycardia, short AV conduction time, and normal QRS complexes reported across 11 cases, but usually attributed to being a variant of Wolff-Parkinson-White syndrome.
1938 – Clerc, Levy and Critesco first described ECG findings of a short PR interval, normal QRS complex, and paroxysmal tachycardia. [Archives des Maladies du Coeur 1938]
1952 – Lown, Ganong and Levine performed the first study correlating the characteristic ECG changes with clinical findings, which distinguished patients with paroxysmal tachycardia, short PR interval, and normal QRS complexes from Wolff-Parkinson-White characteristics. [Circulation 1952]
1961 – Thomas Naum James (1925-2010) described accessory pathway connections between the atria and distal atrioventricular node, which may have a role in the pathophysiology of LGL syndrome [Am Heart J. 1961]
1975 – Brechenmacher described accessory pathways between the atria and bundle of His, which may also be involved in LGL syndrome [Br Heart J. 1975]
Associated Persons
- Bernard Lown (1921)
- William Francis Ganong Jr (1924-2007)
- Samuel Albert Levine (1891-1966)
Alternative Names
- Clerc-Lévy-Cristesco syndrome
- Coronary nodal rhythm syndrome
- Short PQ interval syndrome
- Short PR-normal QRS syndrome
- Short P-R syndrome
References
- Clerc A, Levy R, Critesco C. A propos du raccourcissement permanent de l’espace P-R de l’electrocardiogramme: sans deformation du complexe ventriculaire (About the permanent shortening of the P-R interval on the electrocardiogram: Without deformation of the ventricular complex) Archives des Maladies du Coeur et des Vaisseaux. 1938;31:569–582.
- Wedd AM. Paroxysmal tachycardia, with reference to nomotropic tachycardia and the role of the extrinsic cardiac nerves. Arch Intern Med (Chic). 1921; 27(5):571-590
- Hunter A, Papp C, Parkinson J. The syndrome of short P-R interval, apparent bundle branch block and associated paroxysmal tachycardia. Brit. Heart J. 1940;2: 107-122
- Burch GE, Kimball JL. Notes on the similarity of QRS complex configuration in the Wolff-Parkinson-White syndrome. Am. Heart J. 1946;32: 560
- Littman D. Aberrant auriculoventricular conduction in a patient with paroxysmal tachycardia, a short P-R interval and a normal QRS complex. Am. J. Med. 1947;2: 126
- Söderström N. Observations on the significance of shortened P-R intervals in the electrocardiogram. Cardiologia 1943;7:1–28
- Lown B, Ganong WF, Levine SA. The syndrome of short P-R interval, normal QRS complex and paroxysmal rapid heart action. Circulation. 1952 May;5(5):693-706
- James TN. Morphology of the human atrioventricular node, with remarks pertinent to its electrophysiology. Am Heart J. 1961; 62: 756-771
- Brechenmacher C. Atrio-His bundle tracts. Br Heart J. 1975; 37(8): 853-855
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
eponymictionary
the names behind the name
Doctor in Australia. Keen interest in internal medicine, medical education, and medical history.
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |