
![]()
Waiting Room Medicine
With exponential Emergency Department over-crowding and spiralling waiting times, the Utopian College has produced a series of guidelines to assist fondling members. Ultimately, these Waiting Room guidelines will improve patient comfort and safety; facilitate early diagnosis and treatment (four minute rule) and expedite the global acceptance of Waiting Room Medicine.
Currently, the dyshopian waiting rooms often feel like cold ante-chambers to Hell with reefs of cigarette butts drifting under the non-smoking sign; agonizingly uncomfortable plastic chairs and strange clanking machines that intermittently spit out volcanic black fluid described as coffee, but tasting more like dilute tar.
The Utopian College Council Executive have delegated a task force implementation group sub-committee on Utopian Waiting Room Design. This sub-committee will report to the chief working party liaison group of the Utopian Medicine WorkFlow, which in turn reports to the steering committee of the UberGroups. This should create enough bureaucracy and red-tape to ensure that no suggested implementations in Waiting Room design will ever pass through the bowels of the financial re-design working group or cross the threshold of the ‘almost there‘ implementation committee.
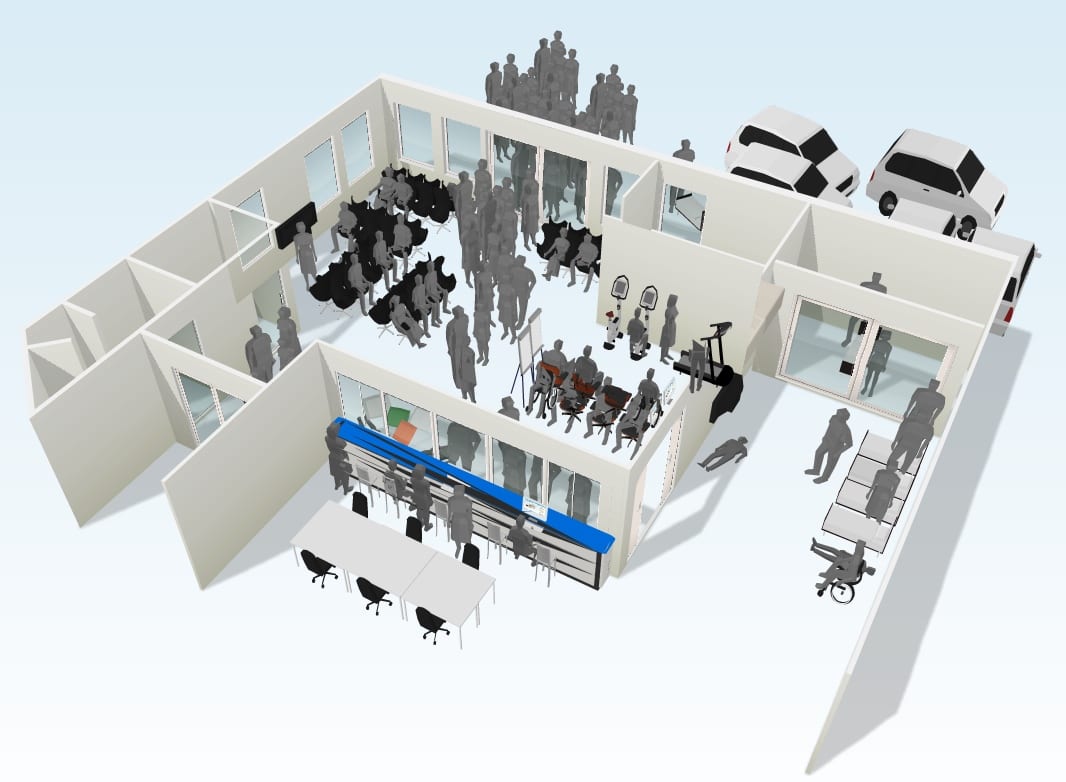
The first draft of the Utopian Waiting Room redesign for the Waiting Room Medicine working party has been published online as a 3D walk-through at and is now available for discussion.
Five discrete areas have been incorporated in the first draft of the Utopian design and are outlined below. Additional areas will include Waiting Room Gynecology, Waiting Room Neurology, Patients without discernible pathology and an area to asses patients for signs of imminent admission…
Feedback in the form of comments, and additional acronyms to be included will be taken into consideration and duly ignored for the second stage of the planning and implementation process. This second stage will coincide with the inaugural Utopian Medicine Conference scheduled to be held on February 29th 2031 in Molvania (details to be announced later this year). The final Waiting Room design will be published in the Journal of Irreproducible Results.
Strategic Areas for Waiting Room Redesign

Coronary Chair Unit (CCU)
Our organized approach to triage and waiting room evaluation for stable chest pain patients is now safe and efficient. Although waiting room evaluation is not ideal, it may be a feasible contingency strategy for periods when ED crowding compromises access to the main department and the use of monitored chairs is required [Reference]
- Monitored chairs are placed in close approximation to, and in sight of, the Triage desk.
- All patients are fitted with defibrillation paddles on arrival and sat around the central defibrillation station.
- Patients then hold hands to create a ‘series’ electrical circuit between the group.
- If a patient develops a shockable rhythm, the circuit is broken and a series of ILCOR derived shocks will be generated to all patients in the circuit.
- Patients deemed to be at risk of imminent collapse should be transferred to the ICU
Imminent Collapse Unit (ICU)
Situated immediately adjacent to the CCU and directly in front of the Triage window. A central clearing of 4m x 4m is covered with strategically placed pillows, blankets and carpeted tiles
Triage is alerted to ICU patients by observing the high-stepping gait of patrons within the queuing community. ICU patient management options are outlined in the UCEM Resuscitation Guidelines V1.07
Geriatric Observation, Mobility and Early Rehabilitation Unit (GOMER)
The GOMER area includes three discrete units
- The Wanderer Containment Unit (WCU) comprises 8-10 doors which open onto each other in a circular arrangement. This ‘Horizontal Hamster wheel‘ helps contain wandering patients without compromising already diluted staff time. Wanderers are able to happily amble in circles for hours without the risk of getting out in to the road or becoming lost in the building.
- Gym distraction area with exercise bikes, treadmills and a selection of ambulatory devices. All floors and flat surfaces are lined with triple thickness EVA foam whilst edges and walls encase pressure triggered inflatable fall arrest soft landing solutions
- Siffre-Time-Fragmentation-Unit (STFU) disengages patients from their environment, and disorientates them with respect to time (length of stay). Utilising the Michel Siffre principle (deprived of light, without time cues, in a room at 20°C, eating the freeze-dried rations of the Apollo 16 program…) patients can adapt to a 48-hour sleep-wake cycle prior to ward admission
Patient Subduement area (PSA)
In dyshopia, the PSA journey starts at triage where conflict, aggression, and abuse is commonplace. Armour plated glass shields the gestalt driven triage nurse as they determine if mist-diffused conversational calmness is required.
A non-blinded single-centre pharma-funded trial of the Agitated Defusion Diffusion Device (ADDD) is underway. Aliquots of aerosolised ‘Eau d’olanzapine®‘ or ‘Midazolam mist®‘ are deployed at 5mg/mL/min as required. Efficacy is measured using the ASS-OL scale (Agitated-Subdued-Sedated-Obtunded-Lethal).

Patients on the ASS end of the scale are led to the PSA, a high walled, sound-proofed section of the waiting room – situated well away from the triage area, playing the UCEM designated Waiting Room Video. Padded chairs, uni-diodotic turnstile entry, soft-tiles, ambient music and lighting are the mainstay of this area.
All PSA areas will be equiped with the latest Defibritazer BP50KV, your one shot answer to electrical restraint and DC cardioversion.
Rarely Assessed or Monitored Patients (RAMP)
- Expandable area (depending upon local policy)
- Comfy seating and refreshments provided for attending ambulance officers; uncomfortable, inappropriately elevated trolleys provided for attending patients
TRIAGE
The TRIAGE area is divided into sections determined largely by the general patient demographic and ability of staff to make up nonsensical acronyms. In this prototype the College have defined consecutive streams of TRIAGE
- Tearful Relatives Inquiring About Getting Examined
- Totally Random Investigation And Granny Emporium
This area provides the ability to
- Administer Utopian medications such as the TTFU pill
- Enable the ‘Say no to Softness‘ border patrol to act
- Prescribe and administer analgesia in a timely manner
- Provide scripts to prevent elopement
- Reduce the length of stay for patients not requiring hospital admission
- Provide a caring environment in the case of mass overdosage
Waiting Room Medicine References:
- Scheuermeyer FX et al. Safety of Assessment of Patients With Potential Ischemic Chest Pain in an Emergency Department Waiting Room: A Prospective Comparative Cohort Study. Ann Emerg Med. 2010 May 23.
- Pines JM et al. The association between emergency department crowding and adverse cardiovascular outcomes in patients with chest pain. Acad Emerg Med. 2009 Jul;16(7):617-25.
- Handel DA et al. The use of scripting at triage and its impact on elopements. Acad Emerg Med. 2010 May;17(5):495-500
- Pines JM et al. The effect of emergency department crowding on analgesia in patients with back pain in two hospitals. Acad Emerg Med. 2010 Mar;17(3):276-83.
- Russ S et al. Placing physician orders at triage: the effect on length of stay. Ann Emerg Med. 2010 Jul;56(1):27-33
UCEM Core Content
- Utopian College of Emergency for Medicine (UCEM)
- UCEM Publications and Position Statements
- UCEM Mission Statement and Essential Roles and Core Competencies
- About the Utopian College. Including Education; Examinations; and Collegial Hierarchy
- Utopian Medicine General News
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |
This is really helpful✊