
![]()
ECG Case 005
The following sequence of ECGs is taken from a middle-aged patient presenting with chest pain and diaphoresis. Can you interpret each ECG tracing in the context of the patient’s symptoms?
ECG 5a – Chest pain and diaphoresis (time = zero)

ECG ANSWER and INTERPRETATION
This ECG demonstrates an evolving anterolateral STEMI:
- ST elevation in V2-5 and aVL
- Reciprocal ST depression in III and aVF
- Pathological Q waves in V2-3
- Hyperacute T waves in V2-4 and I
ECG 5b – Resolution of chest pain (t+20 mins)

ECG ANSWER and INTERPRETATION
There is transient improvement in the ST changes, with development of biphasic T waves in V2-3.
This pattern of T wave changes in V2-3 is known as Wellens syndrome and indicates reperfusion of a previously occluded LAD artery.
The implication of this ECG pattern is that there is an underlying critical LAD stenosis that requires emergent reperfusion, ideally via percutaneous coronary intervention.
ECG 5c – Recurrence of chest pain (t+25 mins)

ECG ANSWER and INTERPRETATION
The previously biphasic T waves are now upright again — this phenomenon is referred to as pseudonormalisation and is a marker of re-occlusion of the culprit artery.
Despite temporary restoration of blood flow in ECG 5b, the patient is now re-infarcting!
ECG 5d – Ongoing chest pain and diaphoresis (t+35 mins)

ECG ANSWER and INTERPRETATION
This ECG demonstrates a frank anterolateral STEMI with evolving ST changes.
This patient had a VF arrest shortly after this ECG was taken, was placed on a mechanical CPR device and taken immediately to the cath lab where she was found to have a 100% proximal LAD occlusion. She was stented, successfully cardioverted and made a good neurological recovery.
CLINICAL PEARLS
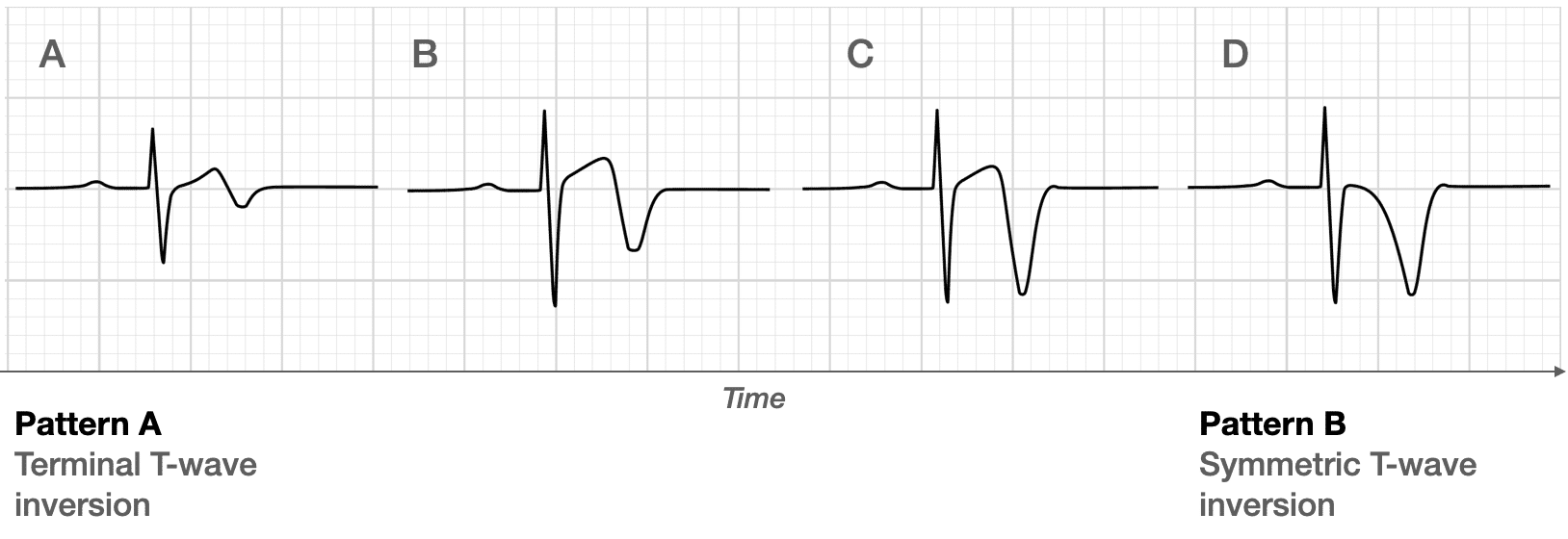
There are two patterns of T-wave abnormality seen in Wellens syndrome:
- Type A – Biphasic, with initial positivity and terminal negativity (25% of cases)
- Type B – Deeply and symmetrically inverted (75% of cases)
These changes evolve with time after reperfusion. The type A pattern is most commonly seen in patients with spontaneous reperfusion of an occluded LAD, as was the case above.
‘Pseudonormalisation’ of T waves may be the first sign of Occlusion Myocardial Infarction (OMI) in patients with Wellens syndrome
Further reading
Related topics
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
TOP 100 ECG Series
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.
Remarkable effort ✨