
![]()
ECG Case 008
70-year old patient presenting with severe chest pain, diaphoresis and syncope. BP 65/40.
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
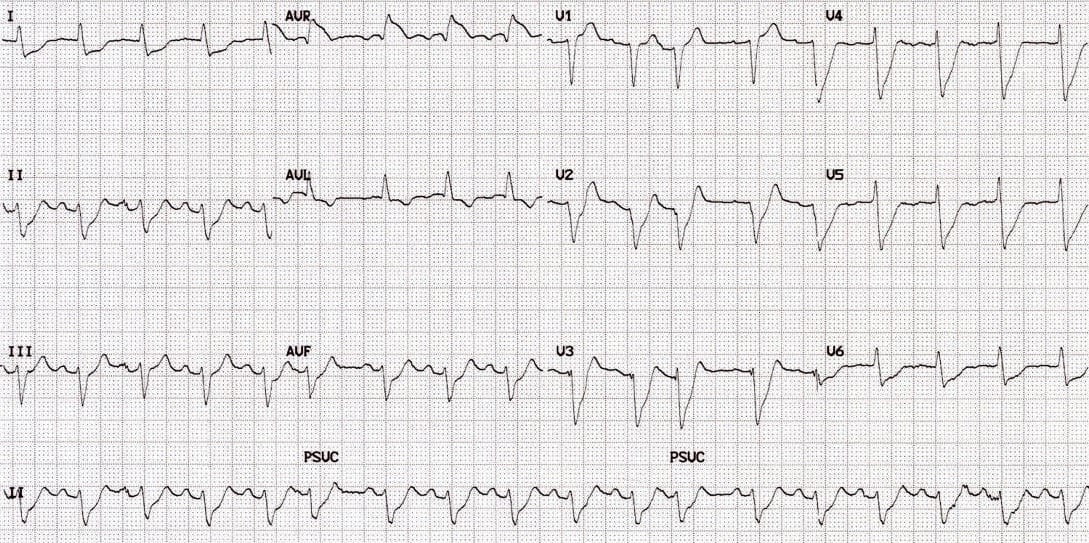
Main Abnormalities
- Widespread ST depression affecting multiple precordial (V2-6) and limb leads (esp. I, II, avF).
- To some extent this is masked by an indistinct J point, upsloping (rather than horizontal) ST depression, and some baseline wander of the ECG
- There is marked ST elevation in aVR, measuring ~3mm
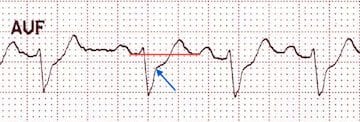
- ST depression in aVF relative to the T-P baseline.
- The blue arrow denotes the approximate position of the J point.
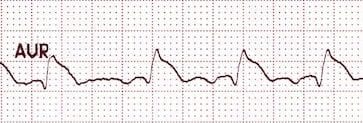
- ST elevation in aVR
Diagnosis
In the context of ischaemic chest pain and cardiogenic shock, the combination of…
- Widespread ST depression
- Marked ST elevation in aVR > 1 mm
- ST elevation in aVR > V1
… is extremely concerning for severe left main coronary artery (LMCA) insufficiency.
However, this pattern is not entirely specific for LMCA insufficiency. It may be seen whenever there is severe diffuse subendocardial ischaemia, as a result of oxygen supply-demand mismatch:
- Severe triple vessel disease
- Severe anaemia or hypoxaemia
- Following resuscitation from cardiac arrest
This patient developed progressive cardiogenic shock complicated by runs of ventricular tachycardia. He was taken for immediate angiography where he was found to have a 99% stenosis of his left main coronary artery.
CLINICAL PEARLS
A similar ECG pattern of diffuse ST depression with ST elevation in aVR may also be seen with supraventricular tachycardias (AVNRT / atrial flutter).
This rate-related change is usually benign and resolves with resolution of the SVT.
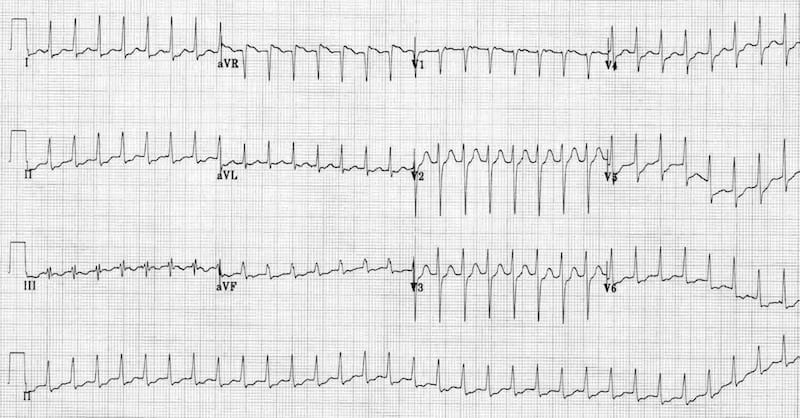
- Rate-related change due to SVT
References
Further Reading
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
TOP 100 ECG Series
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |
Is there any significance to the axis deviation (QRS is positive in avR, biphasic in lead I and negative lead II)?
Also, the wide complex QRS especially in V2-V4?
And the irregularly irregular rhythm (AF)?
Not irregularly irregular rhythm. It is regular, but you can see ectopics with compensatory pause, which makes the ventricular rate look misleadingly irregular.
VW
Agree – In addition to the global STD and STE in aVR I read this as sinus tach. and frequent PAC with marked LAD, PRP and late transition associated with a left anterior hemi block – added observations which probably don’t carry extra clinical significance in the context of LMCA OMI.