
![]()
ST Elevation in aVR
ST elevation in aVR with co-existent multi-lead ST depression indicates subendocardial ischaemia due to O2 supply/demand mismatch.
Clinical causes include:
- Left main coronary artery (LMCA) stenosis
- Proximal left anterior descending artery (LAD) stenosis
- Severe triple vessel disease
- Hypoxia or hypotension, for example following resuscitation from cardiac arrest
ST elevation in aVR can also be seen in the context of anterior STEMI due to LAD occlusion proximal to the first septal branch, causing infarction of the basal septum. Such cases will have associated ST elevation in anteroseptal leads.
Mechanism of ST elevation (STE) in aVR
- Lead aVR is electrically opposite to the left-sided leads I, II, aVL and V4-6. In the case of subendocardial ischaemia, ST elevation in aVR is simply a reciprocal change to ST depression in these leads
- ST depression does not localise, and thus subendocardial ischaemia due to oxygen supply/demand mismatch produces a consistent ECG pattern of widespread ST depression, usually most prominent in leads I, II, V4-6, and reciprocal ST elevation in aVR
- Lead aVR also directly records electrical activity from the right upper portion of the heart, including the right ventricular outflow tract and the basal portion of the interventricular septum. Infarction in this area could theoretically produce ST elevation in aVR
Cause of ST elevation (STE) in AVR
Two possible mechanisms:
- Diffuse subendocardial ischaemia, with widespread ST depression producing reciprocal change in aVR (most common)
- Infarction of the basal septum, i.e. a STEMI involving aVR
The basal septum is supplied by the first septal perforator artery (a very proximal branch of the LAD), so ischaemia / infarction of the basal septum would imply involvement of the proximal LAD.
LMCA “occlusion”: a misnomer
ST elevation in aVR with coexistent multi-lead ST depression can be a sign of Non-Occlusion Myocardial Infarction (NOMI) due to severe single or multi-vessel disease, but does not usually represent acute LMCA occlusion as once thought. Such acute occlusion most often causes sudden cardiac death due to simultaneous anterior, lateral and posterior STEMI.
More recent publications recognise this ECG pattern as consistent with left main coronary artery subocclusion or complete occlusion with well-developed collateral circulation. A 2019 single-centre retrospective analysis identified patients presenting with STE-aVR with multilead ST depression. Coronary occlusion was found only in 10% of patients, and none of these lesions were involving the LAD or left main coronary artery
Predictive Value of STE in aVR
Reveal details
In the context of widespread ST depression + symptoms of myocardial ischaemia:
- STE in aVR ≥ 1mm indicates proximal LAD / LMCA stenosis or severe 3VD
- STE in aVR ≥ 1mm predicts the need for CABG
- Absence of ST elevation in aVR almost entirely excludes a significant LMCA lesion
In the context of anterior STEMI:
- STE in aVR ≥ 1mm is highly specific for LAD occlusion proximal to the first septal branch
In patients undergoing exercise stress testing:
- STE of ≥ 1mm in aVR during exercise stress testing predicts LMCA or ostial LAD stenosis
Magnitude of ST elevation in aVR is correlated with mortality in patients with acute coronary syndromes:
- STE in aVR ≥ 0.5mm was associated with a 4-fold increase in mortality
- STE in aVR ≥ 1mm was associated with a 6- to 7-fold increase in mortality
- STE in aVR ≥ 1.5mm has been associated with mortalities ranging from 20-75%
Deep Dive into the literature of aVR
In-depth review of relevant literature
A Brief Review of the Literature
Over the past 18 years, multiple studies have examined the utility of ST elevation in aVR for predicting severe coronary artery disease (proximal LAD/LMCA/3VD) and mortality in patients with acute coronary syndromes and those undergoing exercise stress testing. Some of the important studies are summarised below…
- Population: 113 patients with unstable angina, including 20 patients with LMCA stenosis and 24 patients with 3VD
- Findings: Patients with LMCA or 3VD frequently demonstrated ST-segment depression in multiple leads (typically I, II and V4-V6) plus ST-segment elevation in lead aVR during attacks of angina
- Population: 100 patients with anterior STEMI
- Findings: STE in aVR of any magnitude was 43% sensitive and 95% specific for LAD occlusion proximal to the first septal branch
- Population: 16 patients with severe LMCA stenosis, 46 patients with acute LAD occlusion and 24 patients with acute RCA occlusion.
- Findings:
- STE in aVR (≥ 0.5mm) occurred with a significantly higher incidence in the LMCA group (88%) than in the LAD (43%) or RCA (8%) groups
- Magnitude of STE in aVR was significantly greater in the LMCA group (1.6 ± 1.3 mm) than the LAD group (0.4 ± 1.0 mm)
- In contrast, magnitude of STE in V1 was less in the LMCA group (0.0 ± 2.1 mm) than in the LAD group (1.4 ± 1.1 mm)
- STE in aVR ≥ V1 distinguished the LMCA group from the LAD group with 81% sensitivity, 80% specificity and 81% accuracy
- Population: 775 patients with first presentation of acute NSTEMI
- Findings:
- Two-thirds of patients with STE in aVR ≥ 1 mm had either LMCA stenosis or severe 3VD
- Degree of STE in aVR was an independent predictor of mortality: STE of ≥ 1 mm was associated with a six- to seven-fold increase in in-hospital mortality (odds ratio of death = 6.6)
- Magnitude of STE in aVR was also closely associated with rates of recurrent ischemic events and heart failure
- STE in aVR predicted the need for CABG – coronary grafting was required in 22% of patients with aVR STE > 1mm compared to 5% of those without
- Population: 150 patients with acute coronary syndromes – 46 with LMCA stenosis, 104 with occlusion of a different vessel
- Findings: STE in aVR was twice as common in patients with LMCA stenosis as those without (69.6% vs 34.6%)
- Population: 310 patients with non-ST-elevation acute coronary syndromes
- Findings:
- STE in aVR ≥ 0.5 mm was the strongest predictor of LMCA or 3VD (78% sensitivity, 86% specificity, 57% PPV and 95% NPV)
- STE in aVR was superior to the presence of ST depression in other leads for predicting LMCA/3VD
- Population: 950 patients with STEMI (any type)
- Findings:
- STE in aVR ≥ 0.5 mm predicted proximal LAD occlusion (with 50% sensitivity, 91% specificity, 55% PPV, 89% NPV).
- STE in aVR ≥ 0.5 mm was also an independent predictor of mortality (in-hospital mortality was 19% in those with ≥ 0.5 mm STE in aVR compared to only 5% in those without).
- Patients with STE in aVR also had higher heart rates, lower systolic BPs, lower ejection fractions and worse Killip class at the time of admission.
- Population: 15, 315 patients with STEMI enrolled in the HERO-2 trial (heparin vs bivalirudin for acute MI)
- Findings: STE ≥1.5 mm in aVR was associated with a two-fold increase in 30-day mortality for both inferior and anterior STEMI, compared to the baseline mortality rate of 10.8%
- Population: 454 patients undergoing both exercise stress testing (standard Bruce protocol) and cardiac catheterization within 6 months, including 75 patients with LMCA or ostial LAD stenosis.
- Findings: STE of ≥ 1mm in aVR during stress testing predicted LMCA or ostial LAD stenosis with sensitivity 75%, specificity 81% and overall accuracy 80%.
- Population: 572 patients with acute NSTEMI
- Findings:
- Degree of STE in aVR was the strongest independent predictor of severe LMCA stenosis / 3VD requiring CABG (odds ratio 29.1), followed by positive troponin T level (odds ratio 1.27).
- STE ≥ 1.0 mm in aVR identified severe LMCA stenosis /3VD with 80% sensitivity, 93% specificity, 56% PPV, and 98% NPV.
ECG Examples
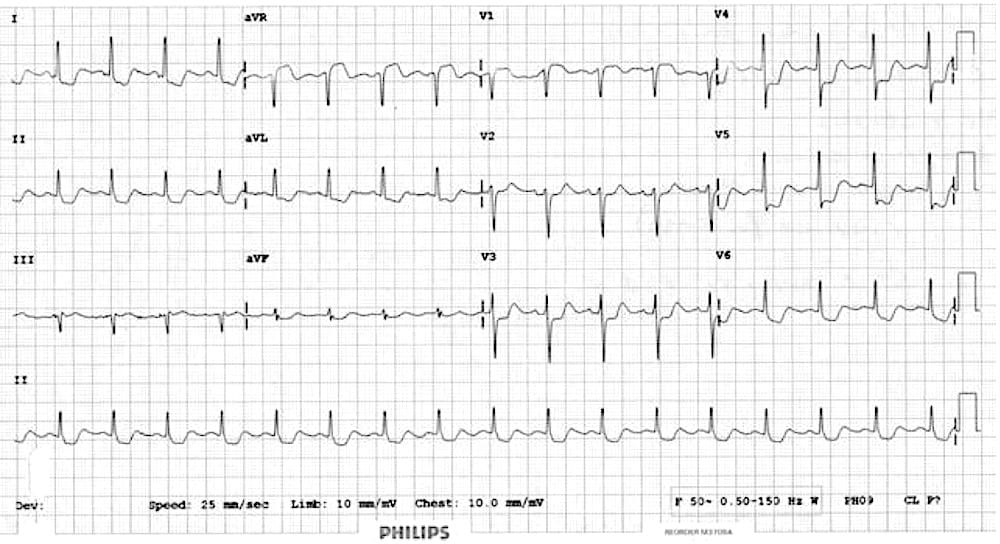
Example 1

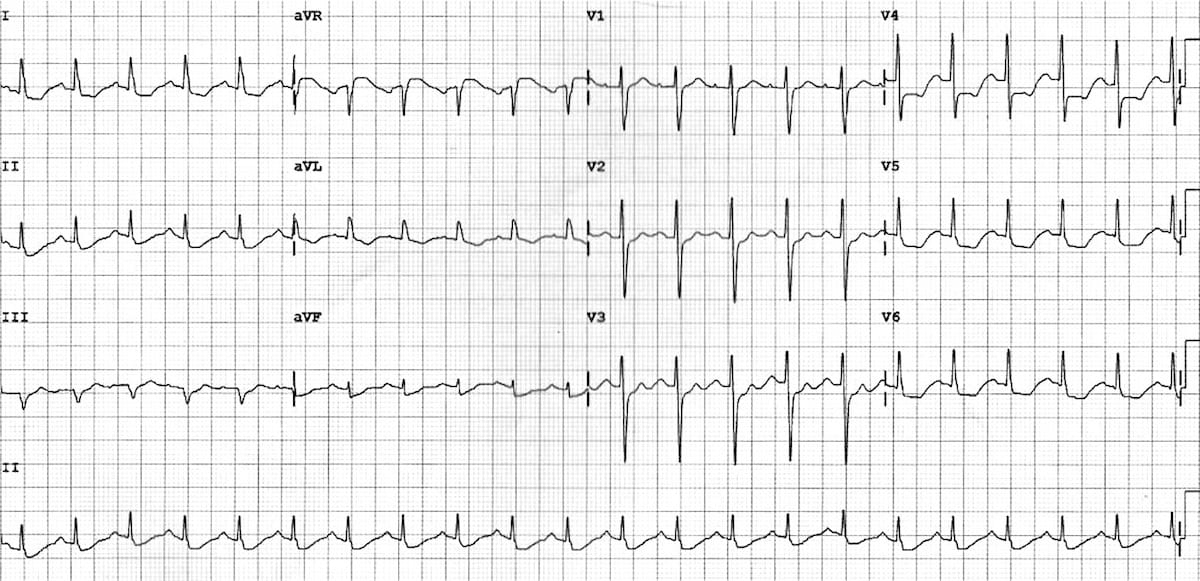
Post cardiac arrest
- Marked ST elevation in aVR which is a reciprocal change to widespread ST depression – even in the presence of a right bundle branch block, ST depression in V2 and V3 is excessively discordant
This ECG was taken 5 minutes post return of spontaneous circulation (ROSC) in a patient who suffered a VF arrest. At this stage, this ECG simply represents oxygen supply-demand mismatch, which is to be expected following extensive down time (20 minutes in this patient).
This patient was taken for angiography which did not reveal acute coronary occlusion.
Note that this ECG will be seen in many patients post-arrest or in the “shocked” patient – although it may represent a degree of underlying coronary artery disease, it does not necessarily indicate occlusion.
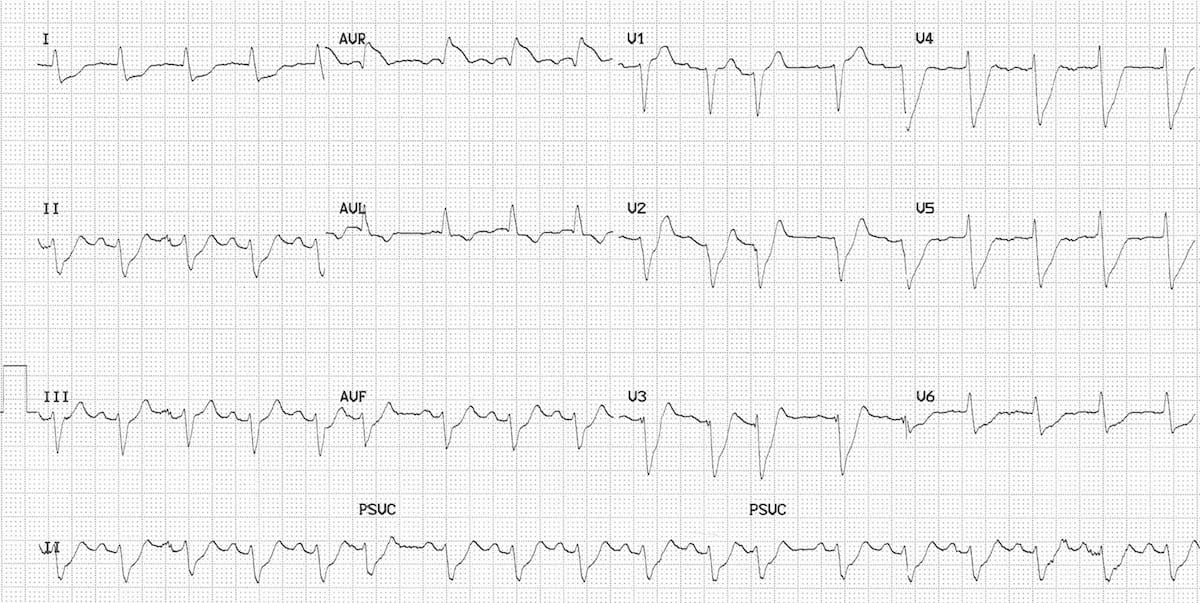
Example 2

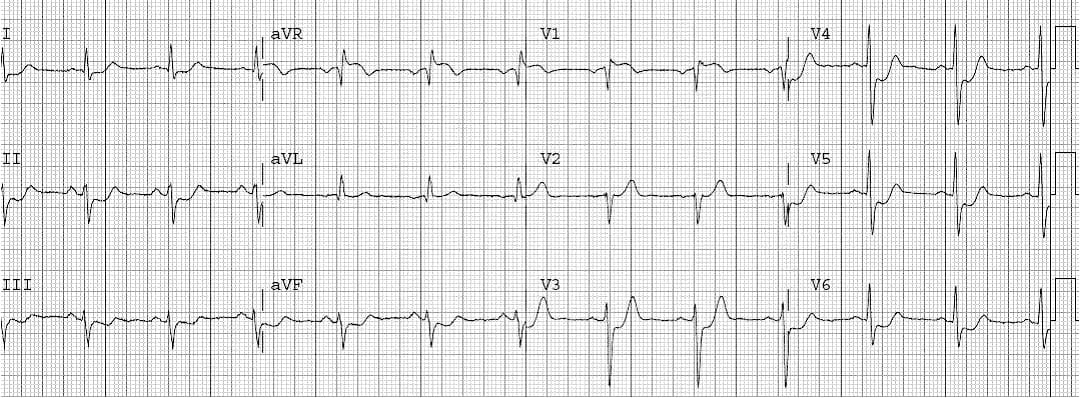
LMCA / 3VD
- Widespread deep ST depression involving V2-6, I, II, aVL
- ST elevation in aVR > V1
The depth and extent of the ST depression indicates severe subendocardial ischaemia
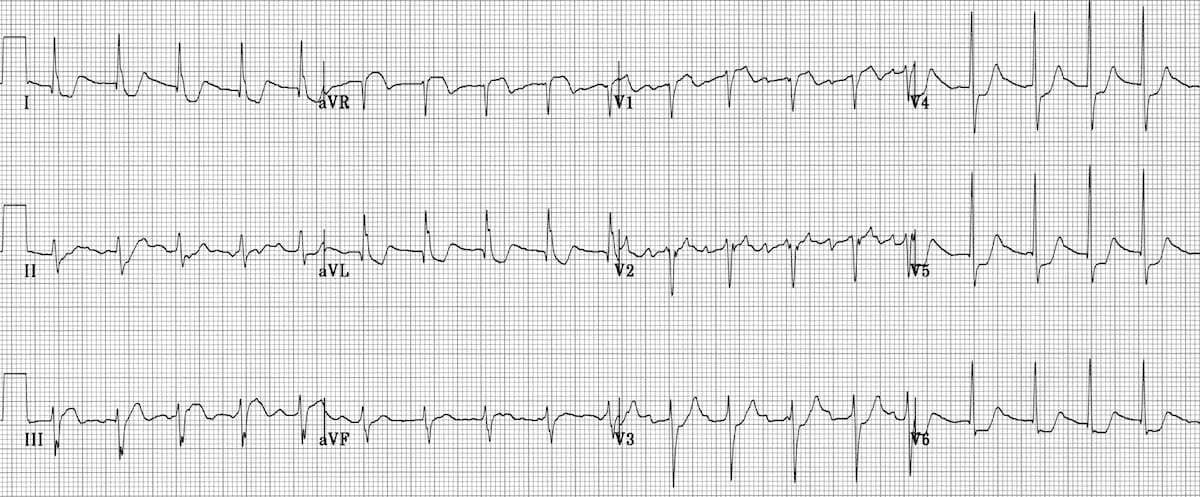
Example 3
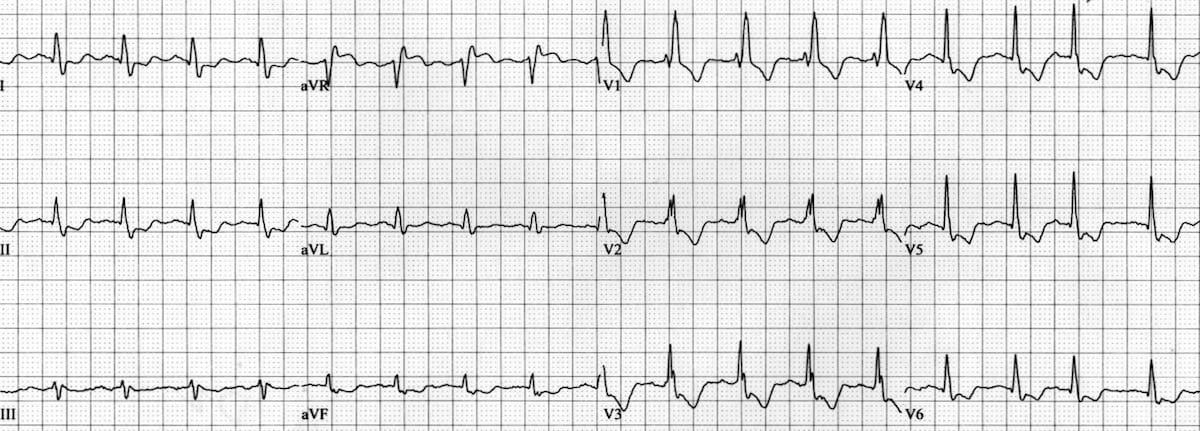
LMCA 95% stenosis
- ST elevation in aVR and V1 of similar magnitude
- Widespread ST depression (V3-6, I, II, III, aVF)
This ECG is reproduced from Dr Smith’s ECG Blog “Head On Motor Vehicle Collision. ST depression. Myocardial Contusion?”
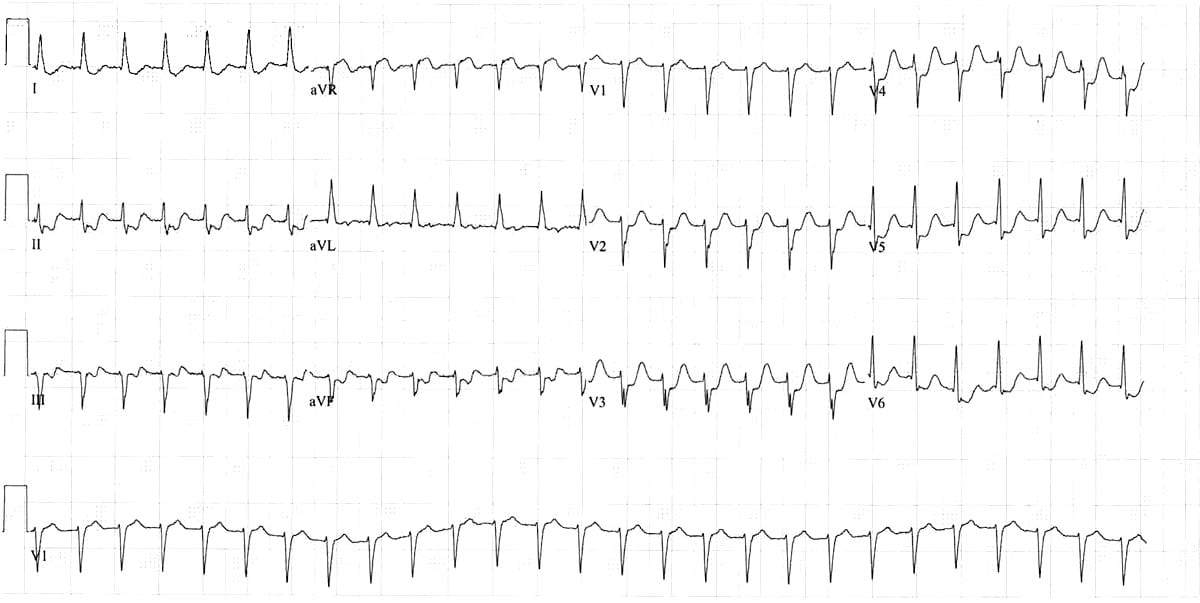
Example 4
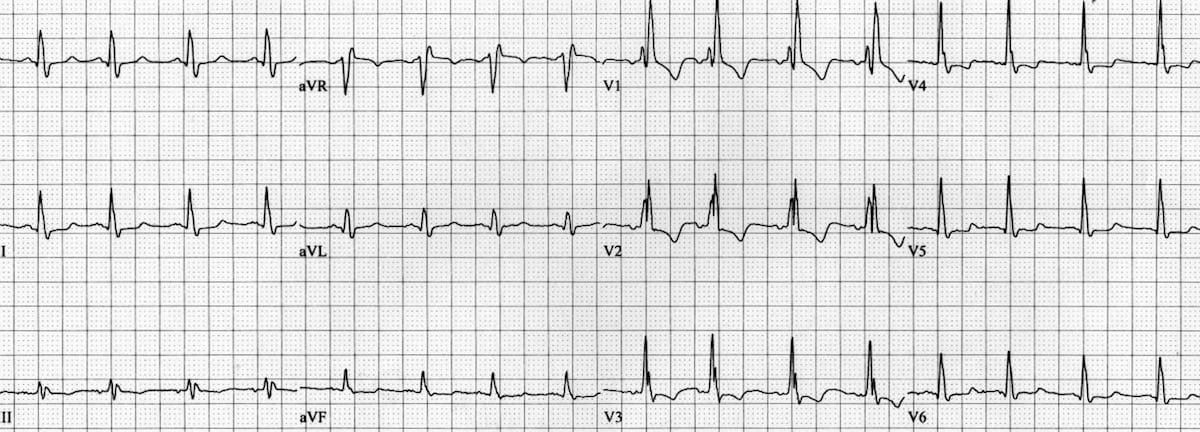
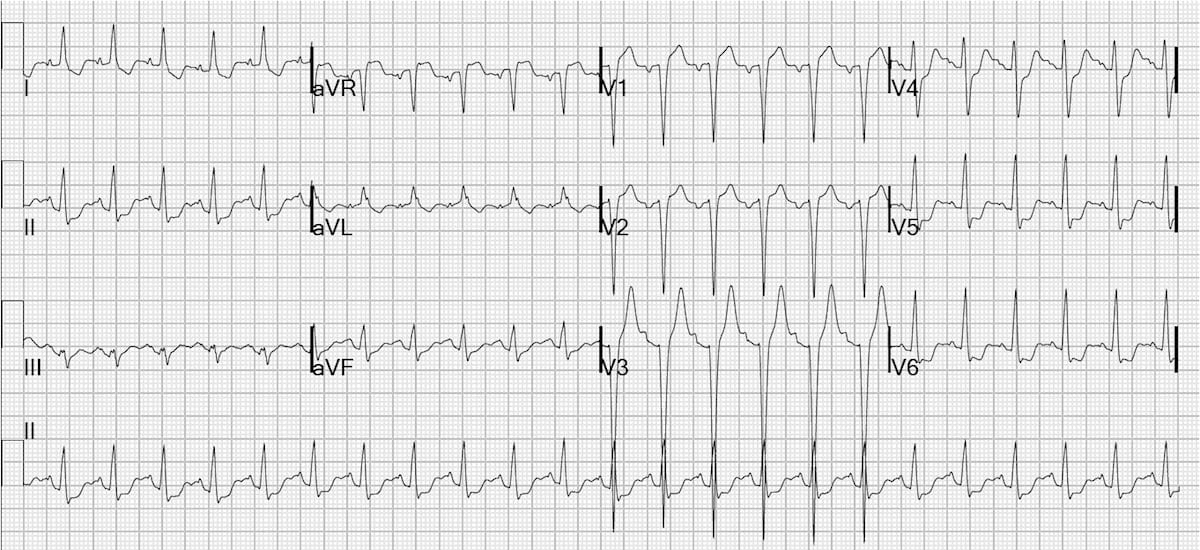
Diffuse subendocardial ischaemia secondary to acute blood loss
- Sinus tachycardia + RBBB
- ST depression in a distribution typical of subendocardial ischaemia (leads V4-6, I, II), with ST elevation in aVR > 1mm
- The ST depression in V1-3 is an expected finding in RBBB, and is therefore more difficult to attribute to ischaemia
This ECG was taken from an elderly man who presented with an acute GI bleed plus chest pain on the background of coronary artery disease. His ischaemic symptoms and ECG improved with blood transfusion.
In this case the subendocardial ischaemia was likely due to cellular hypoxia (O2 supply < demand) from his acute anaemia, exacerbated by poor coronary blood flow.
View Baseline ECG
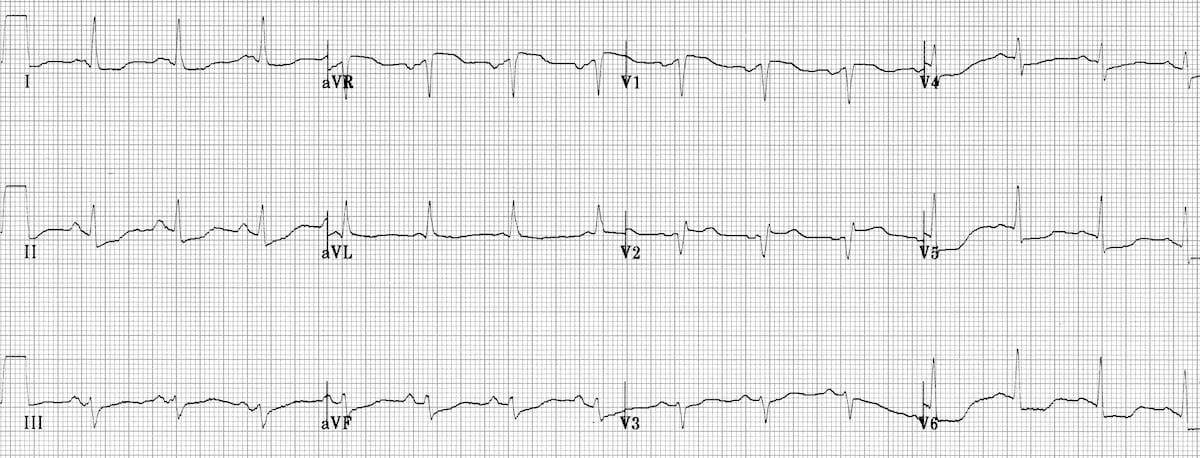
This is the patient’s ECG following blood transfusion and resolution of symptoms. Note:
- Resolving ST depression in V4-6, I, II
- Improved ST depression in V2-3 (initial STD perhaps not entirely due to RBBB then!)
- Resolving ST elevation in aVR
Example 5
Classic example of the LMCA / 3VD ECG pattern:
- Deep horizontal ST depression in multiple leads (V4-6, I, II and aVL)
- ST elevation in aVR + V1
This ECG was contributed by Dr Steve Smith. Read more highly informative blog posts on LMCA stenosis
Example 6
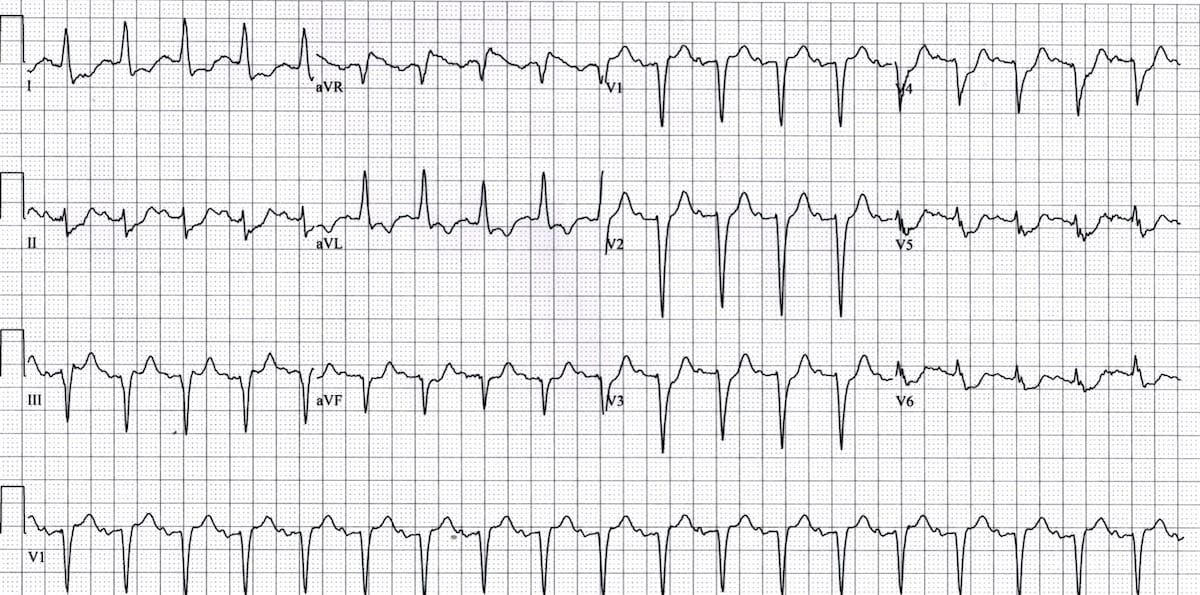
- Sinus tachycardia
- ST elevation in aVR, widespread ST depression (V4-6, I, II, aVL)
- ST elevation in V1 > V2
Aslanger pattern is a specific ECG pattern representing acute inferior occlusion MI (OMI) in patients with concomitant multi-vessel disease. The ST vector of subendocardial ischaemia directed towards aVR can mask inferior ST elevation, with resultant ST elevation only manifesting in lead III. Read more here
Example 7
Severe Multi-Vessel Disease
- ST elevation in aVR and V1, of similar magnitude
- ST depression in multiple leads (V5-6, I, II, aVL, aVF)
- Evidence of anteroseptal STEMI – ST elevation with Q wave formation in V1-3
It would be reasonable to suspect a proximal LAD occlusion based on this ECG. However, this patient actually had severe multi-vessel disease.
Angiography demonstrated a chronic total occlusion of his circumflex artery, with critical stenoses of his proximal LAD, RCA and ramus intermedius. Surprisingly, in this case the culprit vessel was thought to be the RCA, which had been collateralising his chronically occluded circumflex.
Example 8
Proximal LAD Occlusion
- A septal STEMI, with ST elevation and Q wave formation in V1-2
- ST elevation in aVR
- Widespread ST depression, most prominent in leads I, II and V5-6
Given the signs of septal STEMI, this ECG most likely represents a proximal LAD occlusion.
Example 9
LMCA/3VD which demonstrates:
- ST horizontal / downsloping ST depression in multiple leads (V3-6, I, II, aVL)
- ST elevation in aVR > V1
Example 10
LMCA sub-total occlusion
- Marked ST elevation in aVR >> V1
- ST depression in mulitple leads (V2-6, I, II, aVL, aVF), to some extent masked by a non-specific interventricular conduction delay
This patient presented to our ED recently with severe ischaemic chest pain, vomiting, syncope (due to runs of VT) and cardiogenic shock. He was taken for emergent angiography and found to have a sub-total ostial occlusion of his left main coronary artery.
So…is this LMCA stenosis?
This ECG below was originally posted as an example of LMCA stenosis. What do you think?
Reveal Answer
There are some features on this ECG that suggest LMCA/3VD:
- Widespread ST depression, most prominent in the lateral leads (V4-6, I, aVL)
- ST elevation > 1mm in aVR
However, note also:
- Tachycardia
- Flutter waves in V2 — indicating that this patient has atrial flutter with 2:1 block
In this case the ST changes may be due to atrial flutter rather than ischaemia (see below). Thanks to Christopher Watford of EMS 12-lead.com for spotting this one!
Tachycardia-Related ST Depression
Widespread ST depression (with reciprocal STE in aVR) is a common finding in patients with supraventricular tachycardias such as AVNRT or atrial flutter. The significance of this finding in individual patients is unclear, and may be due to:
- Rate-related ischaemia (O2 demand > supply)
- Unmasking of underlying coronary artery disease (i.e. tachycardia as a “stress test”)
- A pure electrical phenomenon (e.g. the young patient with SVT who is relatively asymptomatic and has normal coronary arteries)
ECGs taken following reversion to sinus rhythm will usually show resolution of the ST depression. I would be concerned about underlying coronary artery disease in the following situations:
- ST depression that persists after reversion to sinus rhythm
- Signs of clinical instability – severe chest pain with diaphoresis, hypotension, syncope
- Elevated cardiac biomarkers, with delta troponin rise (NB. a small troponin leak with SVT is common and probably not significant)
- Older patient, multiple cardiac risk factors
Example (a)

Example (b)
Example (c)
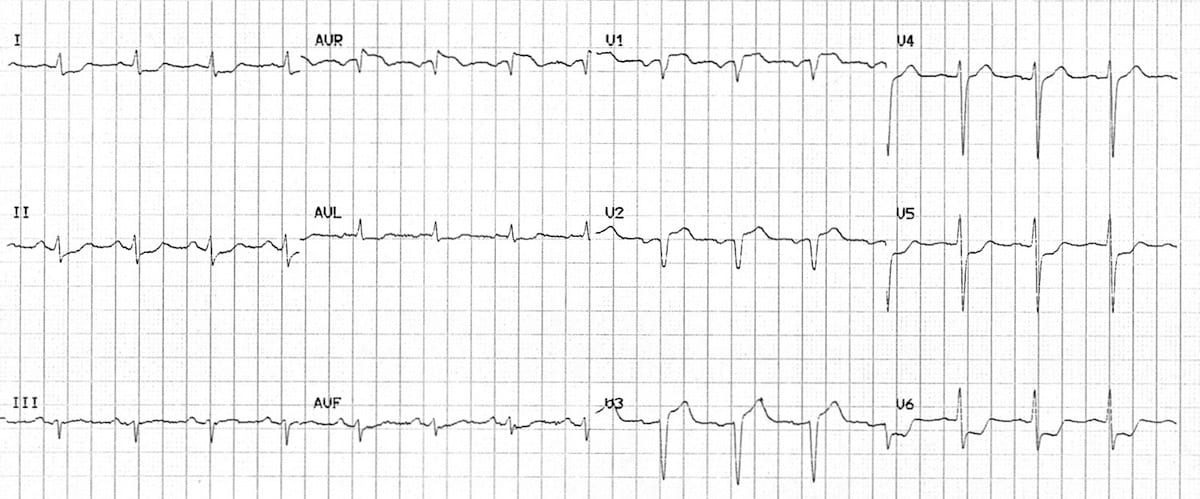
Atrial flutter with rate-related ST depression:
- Tachycardia and flutter waves in V2 indicate atrial flutter with a 2:1 block
- ST depression is seen in I, aVL and V4-6, with reciprocal ST elevation in aVR
Thanks to Christopher Watford of EMS 12-lead.com for spotting this one!
Differential Diagnosis
The differential diagnosis of lateral ST depression includes:
Learn from the FOAM
- Dr Smith’s ECG Blog – STE in aVR
- Dr Smith’s ECG Blog – Left Main Disease
- Salim Rezaie – aVR: The Forgotten 12th Lead
- ECG Guru.com – LMCA case
Related Topics
References
References…there are a lot of them
- Task Force on the management of ST-segment elevation acute myocardial infarction of the European Society of Cardiology (ESC): ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J. 2012 Oct;33(20):2569-619. doi: 10.1093/eurheartj/ehs215
- Aygul N, Ozdemir K, Tokac M, Aygul MU, Duzenli MA, Abaci A et al. Value of lead aVR in predicting acute occlusion of proximal left anterior descending coronary artery and in-hospital outcome in ST-elevation myocardial infarction: an electrocardiographic predictor of poor prognosis. J Electrocardiol. 2008 Jul-Aug;41(4):335-41 [abstract].
- Barrabes JA, Figueras J, Moure C, Cortadellas J, Soler-Soler J. Prognostic value of lead aVR in patients with a first non-ST-segment ele- vation acute myocardial infarction. Circulation 2003; 108: 814 – 819 [full text].
- Chan TC, Brady WJ, Harrigan RA, Ornato JP and Rosen PR. ECG in Emergency Medicine and Acute Care. Elsevier 2005.
- Engelen DJ, Gorgels AP, Cheriex EC, De Muinck ED, Ophuis AJ, Dassen WR et al. Value of the electrocardiogram in localizing the occlusion site in the left anterior descending coronary artery in acute anterior myocardial infarction. J Am Coll Cardiol. 1999 Aug;34(2):389-95 [full text].
- Eskola MJ, Nikus KC, Holmvang L, et al. Value of the 12-lead electrocardiogram to define the level of obstruction in acute anterior wall myocardial infarction: Correlation to coronary angiography and clinical outcome in the DANAMI-2 trial. Int J Cardiol 2009;131:378–383 [abstract].
- Gorgels AP, Engelen DJ, Wellens HJ. Lead aVR, a mostly ignored but very valuable lead in clinical electrocardiography. J Am Coll Cardiol. 2001 Nov 1;38(5):1355-6 [full text].
- Gorgels AP, Vos MA, Mulleneers R, de Zwaan C, Bär FW, Wellens HJ. Value of the electrocardiogram in diagnosing the number of severely narrowed coronary arteries in rest angina pectoris. Am J Cardiol. 1993 Nov 1;72(14):999-1003 [abstract].
- Gul EE, Nikus KC. An unusual presentation of left anterior descending artery occlusion: significance of lead aVR and T-wave direction. J Electrocardiol. 2011 Jan-Feb;44(1):27-30 [full text].
- Hennings JR, Fesmire FM. A new electrocardiographic criteria for emergent reperfusion therapy. Am J Emerg Med. 2011 Jun 22. Epub ahead of print [abstract].
- Jong G, Ma T, Chou P, et al. Reciprocal changes in 12-lead electrocardiography can predict left main coronary artery lesion in patients with acute myocardial infarction. In Heart J 2006;47:13-20 [full text].
- Kireyev D, Arkhipov MV, Zador ST, Paris JA, Boden WE. Clinical utility of aVR-The neglected electrocardiographic lead. Ann Noninvasive Electrocardiol. 2010 Apr;15(2):175-80 [abstract].
- Kosuge M, Ebina T, Hibi K, Endo M, Komura N, Hashiba K et al. ST-segment elevation resolution in lead aVR: a strong predictor of adverse outcomes in patients with non-ST-segment elevation acute coronary syndrome. Circ J. 2008 Jul;72(7):1047-53 [full text].
- Kosuge M, Ebina T, Hibi K, Morita S, Endo M, Maejima N, et al. An early and simple predictor of severe left main and/or three-vessel disease in patients with non-ST-segment elevation acute coronary syndrome. Am J Cardiol. 2011 Feb 15;107(4):495-500 [abstract].
- Kosuge M, Kimura K, Ishikawa T, Ebina T, Shimizu T, Hibi K, et al. Predictors of left main or three-vessel disease in patients who have acute coronary syndromes with non-ST-segment elevation. Am J Cardiol 2005; 95: 1366 – 1369 [abstract].
- Kosuge M, Kimura K, Ishikawa T, Ebina T, Hibi K, Tsukahara K, et al. Combined prognostic utility of ST segment in lead aVR and troponin T on admission in non-ST-segment elevation acute coronary syndromes. Am J Cardiol 2006; 97: 334 – 339 [abstract].
- Kosuge M, Ebina T, Hibi K, Morita S, Komura N, Hashiba K et al. Early, accurate, non-invasive predictors of left main or 3-vessel disease in patients with non-ST-segment elevation acute coronary syndrome. Circ J. 2009 Jun;73(6):1105-10 [full text].
- Kühl JT, Berg RM. Utility of lead aVR for identifying the culprit lesion in acute myocardial infarction. Ann Noninvasive Electrocardiol. 2009 Jul;14(3):219-25 [abstract].
- Nikus KC, Eskola MJ. Electrocardiogram patterns in acute left main coronary artery occlusion. J Electrocardiol. 2008 Nov-Dec;41(6):626-9 [abstract].
- Ozmen N, Yiginer O, Uz O, Kardesoglu E, Aparci M, Isilak Z et al. ST elevation in the lead aVR during exercise treadmill testing may indicate left main coronary artery disease. Kardiol Pol. 2010 Oct;68(10):1107-11 [abstract].
- Pickard AS, Becker RC, Schumock GT, Frye CB. Clopidogrel-associated bleeding and related complications in patients undergoing coronary artery bypass grafting. Pharmacotherapy. 2008 Mar;28(3):376-92 [abstract].
- Rostoff P, Piwowarska W, Konduracka E, Libionka A, Bobrowska- Juszczuk M, Stopyra K, et al. Value of lead aVR in the detection of significant left main coronary artery stenosis in acute coronary syndrome. Kardiol Pol 2005;62:128-37 [abstract].
- Uthamalingam S, Zheng H, Leavitt M, Pomerantsev E, Ahmado I, Gurm GS, Gewirtz H. Exercise-induced ST-segment elevation in ECG lead aVR is a useful indicator of significant left main or ostial LAD coronary artery stenosis. JACC Cardiovasc Imaging. 2011 Feb;4(2):176-86 [abstract].
- de Winter RJ, Verouden NJW, Wellens HJJ, Wilde AAM. A new sign of proximal LAD occlusion. N Engl J Med 2008;359:2071-3 [full text].
- Wiviott SD, Braunwald E, McCabe CH, Montalescot G, Ruzyllo W, Gottlieb S, et al. TRITON-TIMI 38 Investigators. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. 2007 Nov 15;357(20):2001-15 [abstract].
- Williamson K, Mattu A, Plautz CU, Binder A, Brady WJ. Electrocardiographic applications of lead aVR. Am J Emerg Med. 2006 Nov;24(7):864-74 [pdf].
- Wong CK, Gao W, Stewart RA, French JK, Aylward PE, White HD; for the HERO-2 Investigators. The prognostic meaning of the full spectrum of aVR ST-segment changes in acute myocardial infarction. Eur Heart J. 2011 Aug 19 [abstract].
- Yamaji H, Iwasaki K, Kusachi S, Murakami T, Hirami R, Hamamoto H, et al. Prediction of acute left main coronary artery obstruction by 12-lead electrocardiography. ST segment elevation in lead aVR with less ST segment elevation in lead V(1). J Am Coll Cardiol. 2001 Nov 1;38(5):1348-54 [full text].
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
ECG LIBRARY
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.
Hi, I’m a cardiology trainee and have frequently seen avr elevation and global depression in cases of out of hospital cardiac arrest . Initial rhythm with ambos is PEA, which is a bad sign and a potential clue to non ischaemic origin. CT head revealed non survivable SAH. Avr elevation has a broad differential and one that shouldn’t trigger immediate Cath lab activation