
![]()
Atrial Flutter
ECG features of atrial flutter
- Narrow complex tachycardia
- Regular atrial activity at ~300 bpm
- Loss of the isoelectric baseline
- “Saw-tooth” pattern of inverted flutter waves in leads II, III, aVF
- Upright flutter waves in V1 that may resemble P waves
- Ventricular rate depends on AV conduction ratio (see below)
Note: the above pattern of inverted flutter waves in inferior leads and upright flutter waves in V1 occurs in atrial flutter due to anticlockwise reentry, which makes up 90% of cases.
Fixed AV conduction ratio (“AV block”)
Ventricular rate is a fraction of the atrial rate, for example:
- 2:1 block = 150 bpm
- 3:1 block = 100 bpm
- 4:1 block = 75 bpm
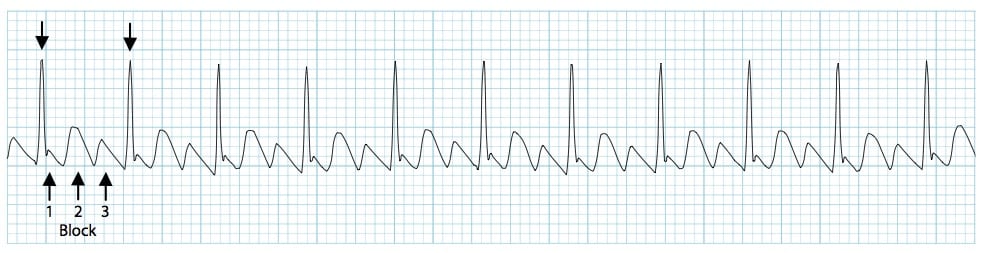
Variable AV conduction ratio
- The ventricular response is irregular and may mimic atrial fibrillation (AF)
- On closer inspection, there may be a pattern of alternating 2:1, 3:1 and 4:1 conduction ratios
Pathophysiology of atrial flutter
Atrial flutter is a form of supraventricular tachycardia caused by a re-entry circuit within the right atrium. The length of the re-entry circuit corresponds to the size of the right atrium, resulting in a fairly predictable atrial rate of around 300 bpm (range 200-400)
- Ventricular rate is determined by the AV conduction ratio (“degree of AV block”). The most common AV ratio is 2:1, resulting in a ventricular rate of ~150 bpm
- Higher-degree blocks can occur — usually due to medications or underlying heart disease — resulting in lower rates of ventricular conduction, e.g. 3:1 or 4:1 block.
- Atrial flutter with 1:1 conduction can occur due to sympathetic stimulation, or in the presence of an accessory pathway. The administration of AV-nodal blocking agents to a patient with Wolff-Parkinson-White syndrome can precipitate this
- Atrial flutter with 1:1 conduction is associated with severe haemodynamic instability and progression to ventricular fibrillation
NB. The term “AV block” in the context of atrial flutter is something of a misnomer. AV block is a physiological response to rapid atrial rates and implies a normally functioning AV node.
Classification
This is based on the anatomical location and direction of the re-entry circuit.
Typical atrial flutter (common)
Sometimes known as type I flutter, this involves the IVC & tricuspid isthmus in the reentry circuit. Further classified based on the direction of the reentry circuit (anticlockwise or clockwise):
Anticlockwise Reentry: Commonest form of atrial flutter (90% of cases). Retrograde atrial conduction produces:
- Inverted flutter waves in leads II,III, aVF
- Positive flutter waves in V1 — may resemble upright P waves
Clockwise Reentry: This uncommon variant produces the opposite pattern:
- Positive flutter waves in leads II, III, aVF
- Broad, inverted flutter waves in V1
Learn more about the mechanism behind “anticlockwise” and “clockwise” reentry…
- Interatrial conduction during normal sinus rhythm occurs via Bachmann’s bundle (BB), the fossa ovalis, and the coronary sinus os
- Whilst patterns of interatrial conduction in atrial flutter are less well established, they are thought to occur via similar pathways
- In both forms of typical atrial flutter, the reentrant circuit is formed in the right atrium. The left atrium is passively activated and is not necessary to maintain the tachycardia
Anticlockwise reentry

- Anticlockwise reentry circuit forms in the right atrium
- Interatrial conduction and subsequent left atrial activation occurs via Bachman’s bundle (BB) and the coronary sinus os
- The anticlockwise nature of the reentry circuit means that interatrial conduction occurs first via the coronary sinus os, and later via BB
- The majority of left atrial conduction and activation thus occurs in a retrograde manner, forming negative flutter waves in inferior leads
Clockwise reentry

- Clockwise reentry circuit forms in the right atrium
- Interatrial conduction occurs via the same pathways, with left atrial activation now occurring first via BB
- The majority of left atrial activation occurs in an anterograde manner, forming positive flutter waves in inferior leads
Atypical atrial flutter (uncommon)
- Sometimes referred to as type II flutter, does not fulfill criteria for typical atrial flutter
- Often associated with higher atrial rates and rhythm instability
- Less amenable to treatment with ablation
Handy Tips For Spotting Flutter
Rapid Recognition
- Narrow complex tachycardia at 150 bpm (range 130-170)? Yes -> Suspect flutter!
- Turn the ECG upside down and closely examine the inferior leads (II, III + aVF) for flutter waves
Vagal Manoeuvres +/- Adenosine
- Atrial flutter will not usually cardiovert with these techniques (unlike AVNRT), although typically there will be a transient period of increased AV block during which flutter waves may be unmasked
RR intervals
- In atrial flutter with variable block the R-R intervals will be multiples of the P-P interval — e.g. assuming an atrial rate of 300bpm (P-P interval of 200 ms), the R-R interval would be 400 ms with 2:1 block, 600 ms with 3:1 block, and 800 ms with 4:1 block
- Look for identical R-R intervals occurring sporadically along the rhythm strip; then look to see whether there is a mathematical relationship between the various R-R intervals on the ECG
- In contrast, atrial fibrillation will be completely irregular, with no patterns to be discerned within the R-R intervals
ECG Examples
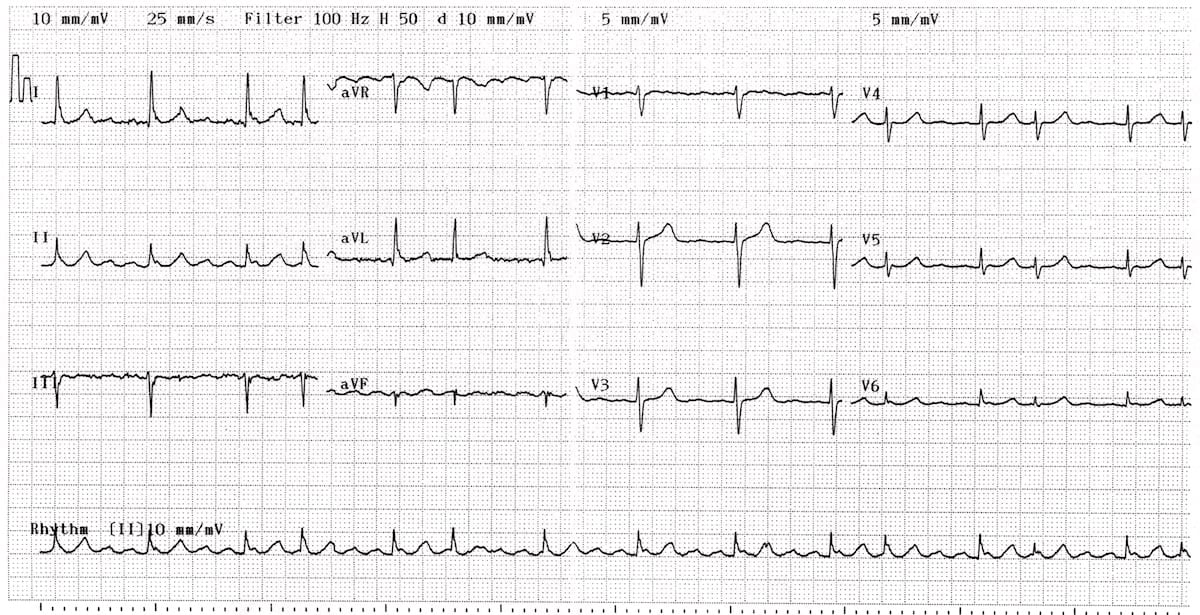
Example 1
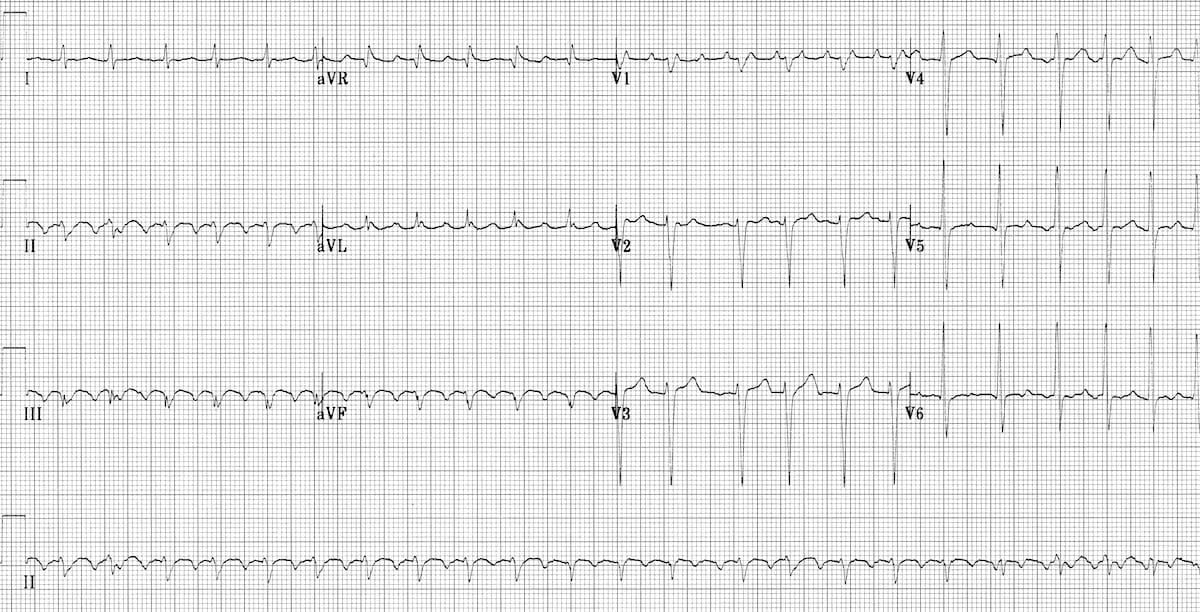
Atrial Flutter with 2:1 Block
This is the classic appearance of anticlockwise flutter:
- Inverted flutter waves in II, III + aVF at a rate of 300 bpm (one per big square)
- Upright flutter waves in V1 simulating P waves
- 2:1 AV block resulting in a ventricular rate of 150 bpm
- Note the occasional irregularity, with a 3:1 cycle seen in V1-3
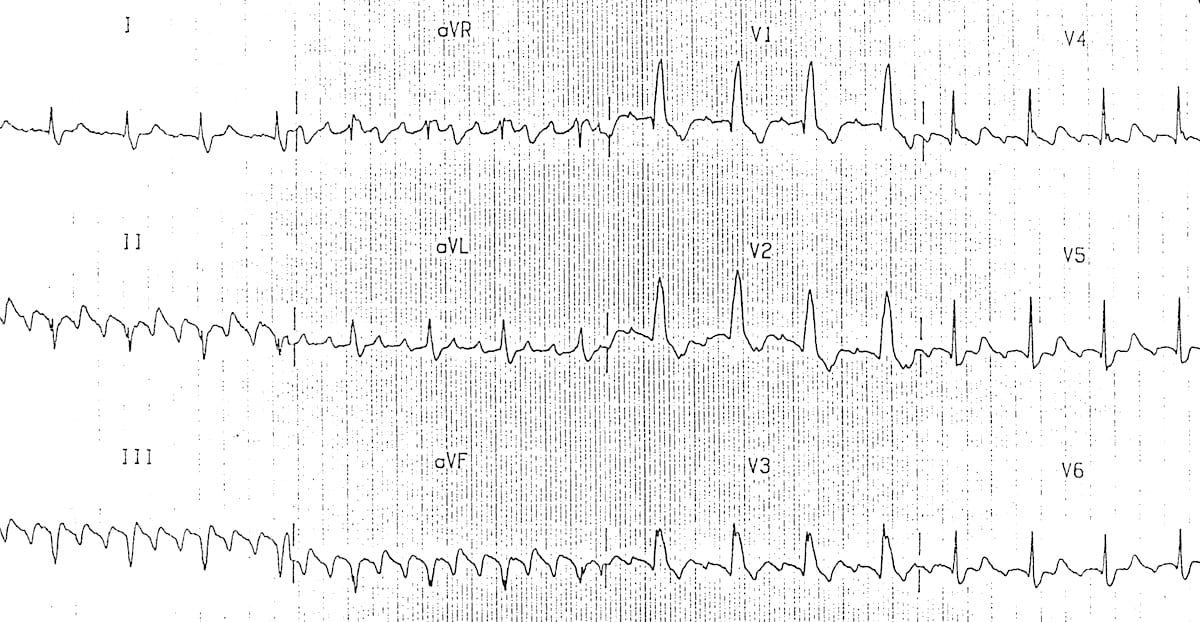
Example 2
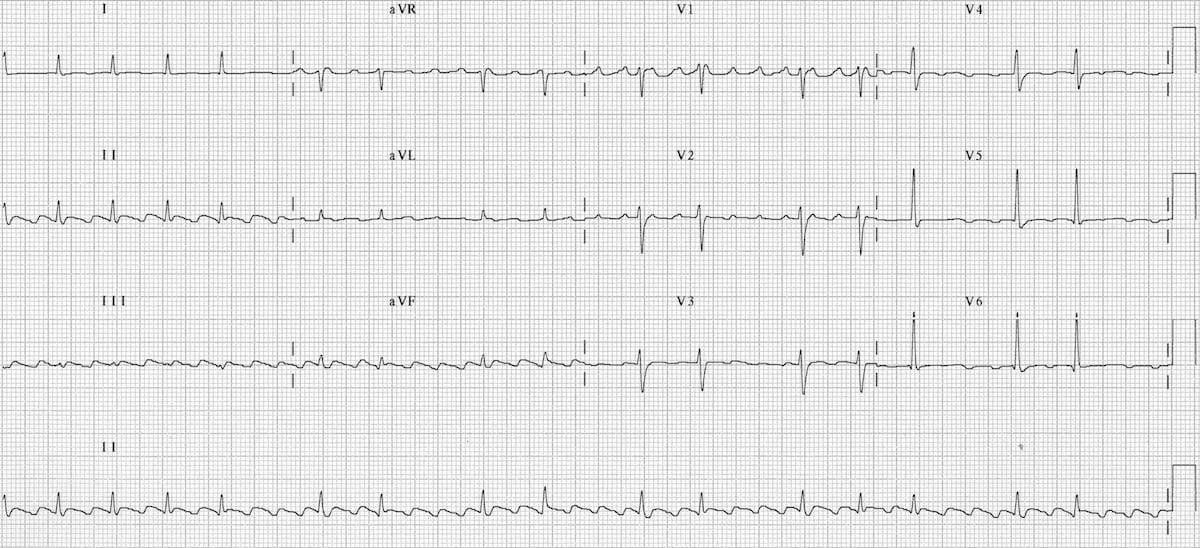
Atrial flutter with variable block
- Inverted flutter waves in II, III + aVF with atrial rate ~ 300 bpm
- Positive flutter waves in V1 resembling P waves
- The degree of AV block varies from 2:1 to 4:1
The diagnosis of flutter with variable block could be inferred here from the R-R intervals alone (e.g. if flutter waves were indistinct) — note how the R-R intervals during periods of 4:1 block are approximately double the R-R intervals during 2:1 block.
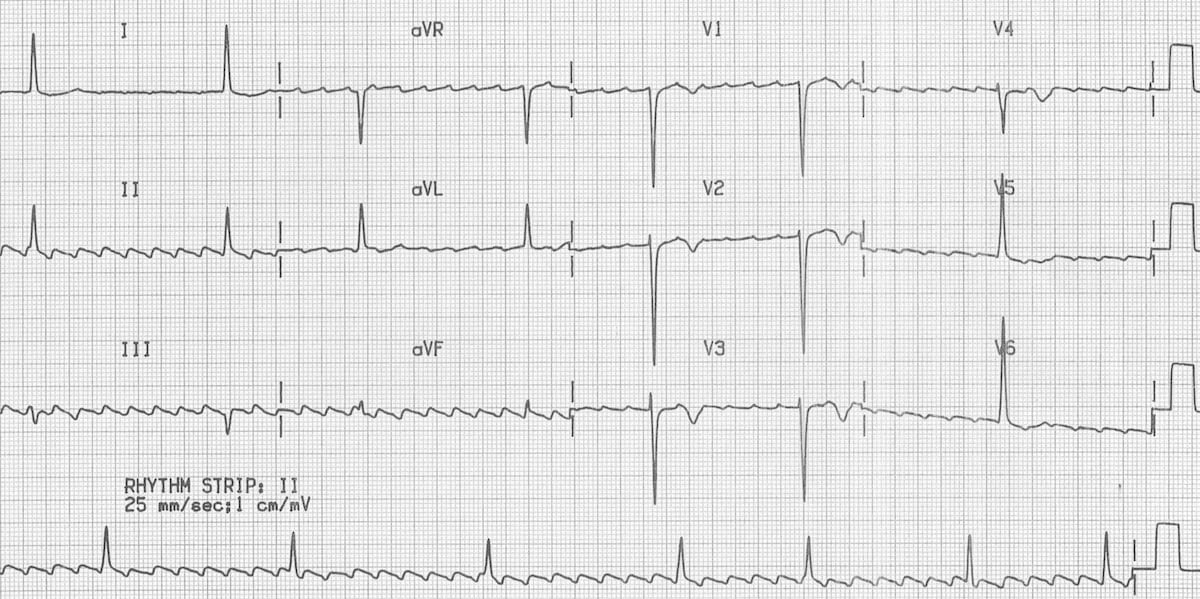
Example 3
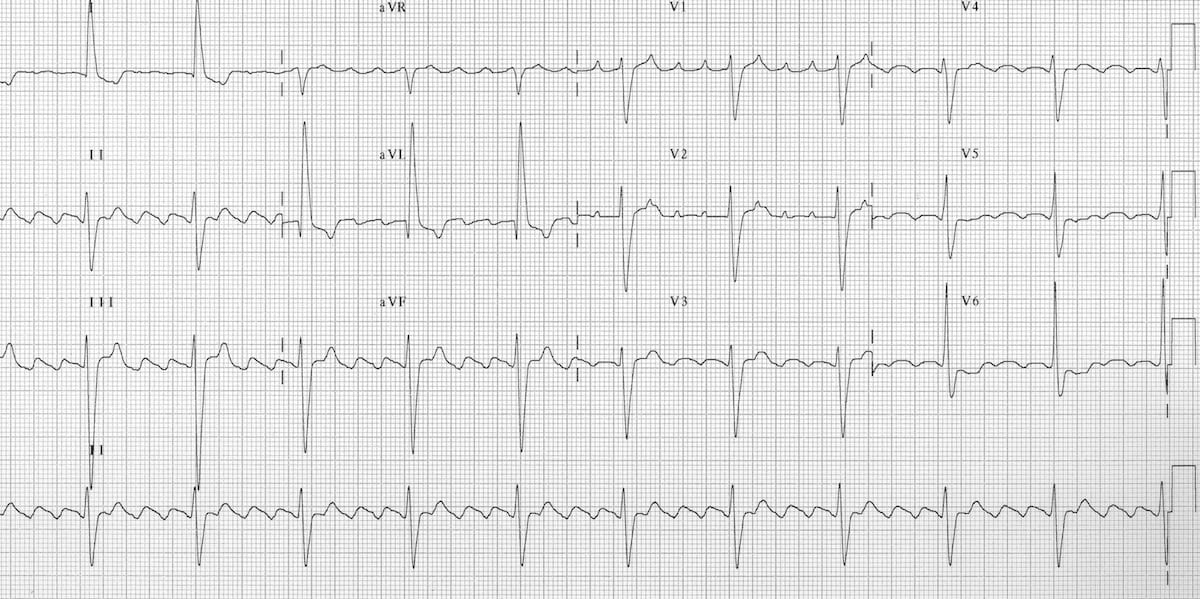
Atrial flutter with 4:1 block
- There are inverted flutter waves in II, III + aVF at a rate of 260 bpm
- There are upright flutter waves in V1-2 (= anticlockwise circuit)
- There is 4:1 block, resulting in a ventricular rate of 65 bpm
- The relatively slow ventricular response suggests treatment with an AV nodal blocking agent
Example 4
Atrial Flutter with Variable Block
- The block varies between 2:1 and 4:1
- The presence of positive flutter waves in lead II suggests a clockwise re-entry circuit (= uncommon variant)
Example 5
Atrial Flutter with High-Grade AV Block
- There is anticlockwise flutter with marked AV block (varying from 5:1 up to 8:1)
- The very low ventricular rate suggests treatment with AV nodal blocking drugs (e.g. digoxin, beta-blockers)
- Other possibilities could include intrinsic conducting system disease (true “AV block”) or electrolyte abnormality (e.g. hyperkalaemia)
Note: The combination of new-onset atrial flutter with high-grade AV block is very suspicious for digoxin toxicity
Example 6
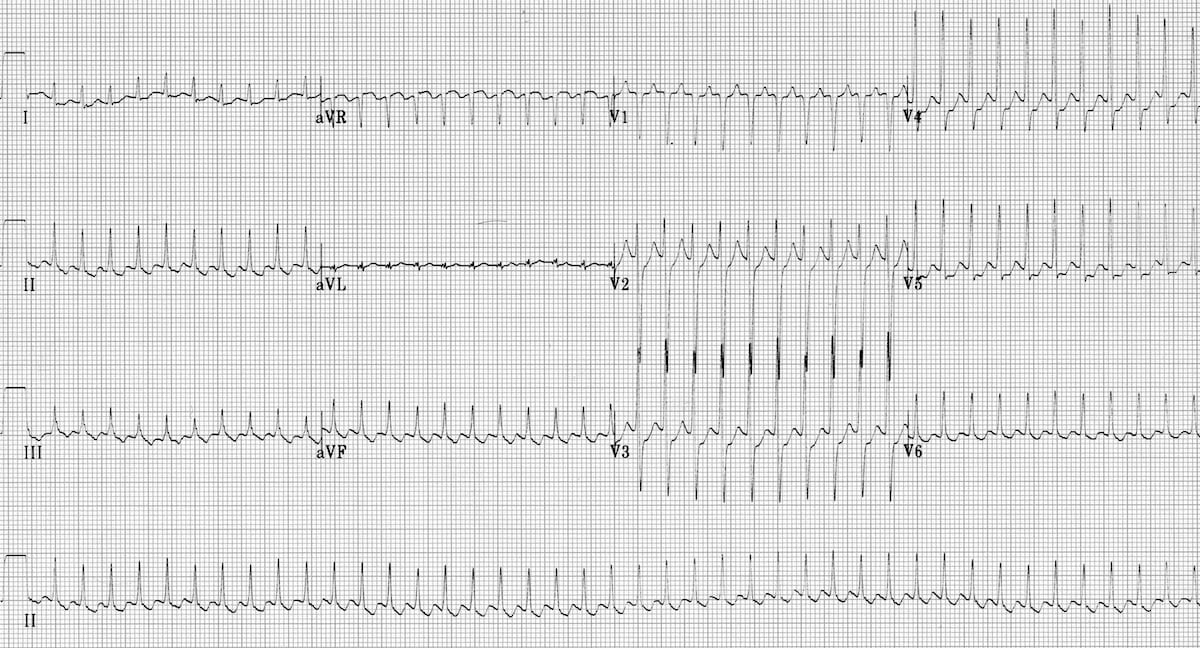
Atrial Flutter with 1:1 Block
- There is a very rapid, regular narrow-complex tachycardia at 250-300 bpm
- Flutter waves are not clearly seen, but there is an undulation to the baseline in the inferior leads suggestive of flutter with a 1:1 block
- Alternatively, this may just be rapid SVT (AVNRT/AVRT) with rate-related ST depression
With ventricular rates as rapid as this, spending any further time evaluating the ECG is unwise! Resuscitation is the priority… This patient will almost certainly be haemodynamically unstable, requiring emergent DC cardioversion.
Example 7
Atrial Flutter with 2:1 Block
- Narrow complex tachycardia at 150 bpm
- There are no visible P waves
- Sawtooth baseline in V1 with flutter waves visible at 300 bpm
- Elsewhere, flutter waves are concealed in the T waves and QRS complexes
- The heart rate of 150 bpm makes this flutter with a 2:1 block
NB. Flutter waves are often very difficult to see when 2:1 block is present.
Remember…
- Suspect atrial flutter with 2:1 block whenever there is a regular narrow-complex tachycardia at 150 bpm — particularly when the rate is extremely consistent
- In contrast, the rate in sinus tachycardia typically varies slightly from beat to beat, while in AVNRT/AVRT the rate is usually faster (170-250 bpm)
- To differentiate between these rhythms, try some vagal manoeuvres or give a test dose of adenosine — AVNRT/AVRT will often revert to sinus rhythm, whereas slowing of the ventricular rate will unmask the underlying atrial rhythm in sinus tachycardia or atrial flutter


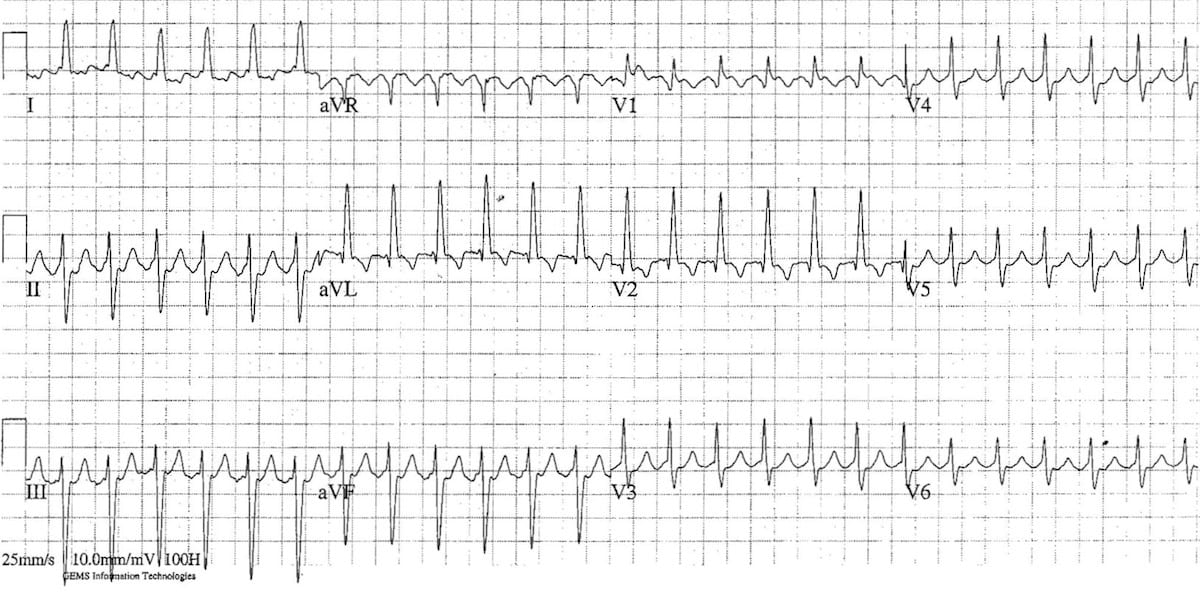
Example 8
Atrial flutter with 3:1 Block
- Negative flutter waves at ~ 300bpm are best seen in the inferior leads II, III and aVF (= anticlockwise pattern)
- There is a 3:1 relationship between the flutter waves and the QRS complexes, resulting in a ventricular rate of 100 bpm
Related Topics
References
- Dr Smith’s ECG Blog – Atrial Flutter
- Rob Orman @ ERCast – Atrial Flutter, Fibrillation and Ablation (podcast)
- Saoudi N, Cosío F, Waldo A, Chen SA, Iesaka Y, Lesh M, Saksena S, Salerno J, Schoels W; Working Group of Arrhythmias of the European of Cardiology and the North American Society of Pacing and Electrophysiology. A classification of atrial flutter and regular atrial tachycardia according to electrophysiological mechanisms and anatomical bases; a Statement from a Joint Expert Group from The Working Group of Arrhythmias of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Eur Heart J. 2001 Jul;22(14):1162-82. PMID: 11440490 Full Text
- Wells JL Jr, MacLean WA, James TN, Waldo AL. Characterization of atrial flutter. Studies in man after open heart surgery using fixed atrial electrodes. Circulation. 1979 Sep;60(3):665-73. PMID: 455626 Full Text
- Marine et al. Different Patterns of Interatrial Conduction in Clockwise and Counterclockwise Atrial Flutter. Circulation. 2001;104:1153–1157
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
ECG LIBRARY
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.
This was a great article. I’ve got a Zoll on my desk with an EKG trainer and have been scratching my head at Flutter for awhile now – thank you for this contribution! -Jesse
How to diference afib from aflutter w irregular response?
you may notice an alternating pattern of 2:1, 3:1 and 4:1 block (2 flutter waves for 1 QRS, 3 flutter waves for 1 QRS and 4 flutter waves for 1 QRS) between the beats just like in example 2 in lead II.