
![]()
ECG Case 007
70-year old patient presenting with chest pain, dyspnoea and dizziness. BP 90/50. SaO2 83% RA
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
Main Abnormalities
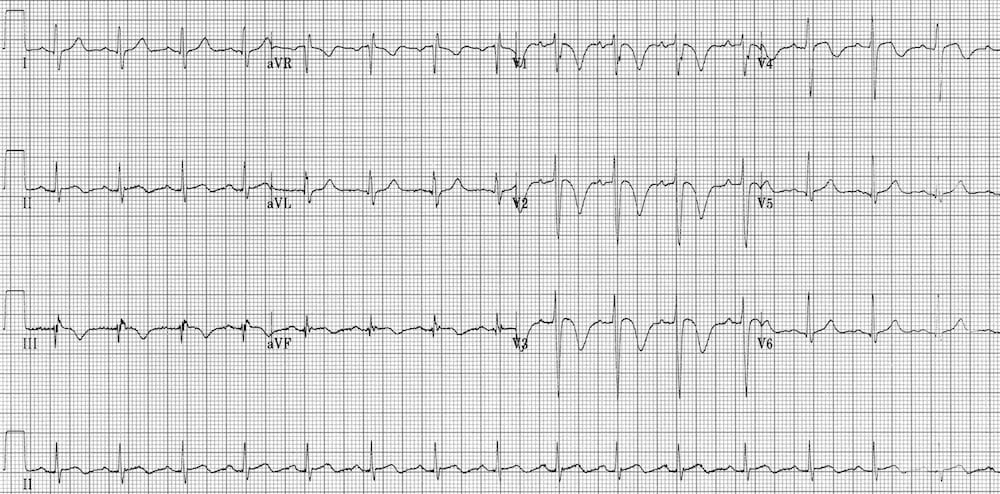
- Sinus tachycardia ~ 100 bpm
- Anterior T wave abnormalities: inverted in V1-4
- Inferior T wave abnormalities: inverted in III, aVF
- Subtle ST elevation in III and aVF, without reciprocal changes
Significance of ECG Findings
This pattern of T wave inversions in the right precordial leads V1-4 plus the inferior leads (especially the rightward-facing lead III) is referred to as the right ventricular strain pattern. It is a marker of right ventricular hypertrophy or dilatation.
Diagnosis
In a patient presenting with acute shortness of breath, the combination of…
- Sinus tachycardia
- RV strain pattern in V1-4 (+/- lead III)
… is highly suggestive of acute cor pulmonale due to massive pulmonary embolism.
However, these ECG changes are not specific to PE and may be seen in other conditions associated with pulmonary hypertension and RV enlargement including:
- Chronic lung disease (COPD, lung fibrosis) with chronic cor pulmonale
- Right ventricular hypertropy — e.g. due to congenital causes, valvular heart disease
- Arrhythmogenic right ventricular cardiomyopathy
CLINICAL PEARLS
Anterior T-wave inversion in V1-3 is also seen in Wellens syndrome. The presence of concurrent inferior T-wave inversion, especially in leads facing the right ventricle (III), is highly specific for differentiating pulmonary embolism from Wellens syndrome. For another example of this pattern, see ECG Case 123.
Other ECG findings associated with pulmonary embolism include:
- New right axis deviation
- New right bundle branch block
- New dominant R wave in V1
- Non-specific ST segment changes
The often quoted SI QIII TIII pattern (deep S wave in lead I, Q wave in III, inverted T wave in III) is neither sensitive nor specific for PE and is infrequently seen (20% of cases).
Similarly, sinus tachycardia is not as ubiquitous in PE as people seem to think (< 50% of cases), and certainly should not be relied up to exclude PE.
References
Further Reading
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
TOP 100 ECG Series
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |
How to differentiate this from Wellens-Syndrom?
The presence of concurrent TWI in inferior leads, especially III facing the RV, is highly specific for differentiating PE from Wellens. See https://litfl.com/ecg-case-123/ for another great example of this. ECG changes in Wellens will also usually be dynamic.
any mention of those funky p waves?
i can also see S1Q3T3, am i right ?
I can see R-R´ in DIII