
![]()
ECG Case 026
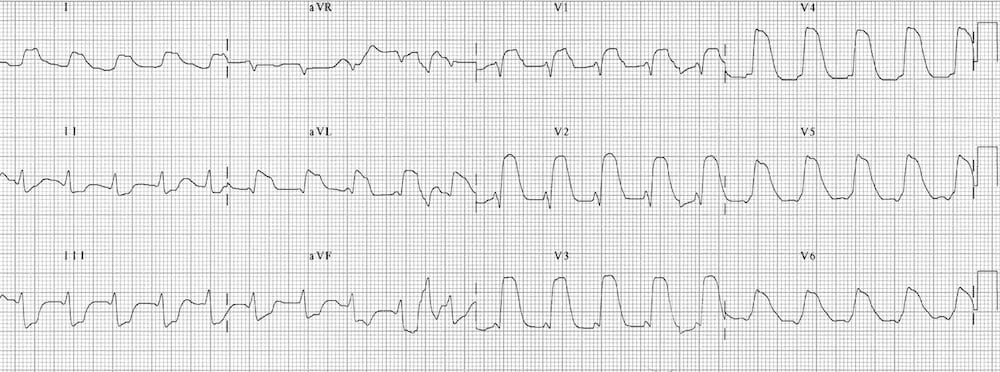
70-year old patient presenting with chest pain and diaphoresis. Describe the ECG.
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
This is a very worrying ECG demonstrating massive anterolateral STEMI with “tombstone” morphology:
- Gross ST elevation in V1-6, I and aVL
- Early Q wave formation in aVL
- Reciprocal ST depression in inferior leads II, III and aVF
This ECG pattern is seen in proximal LAD occlusion and indicates a large territory infarction with a poor LV ejection fraction. These patients are at high likelihood of ventricular fibrillation (VF), cardiogenic shock and death, and require aggressive management both pre-hospital and in the emergency department setting.
CLINICAL PEARLS
Check out the other “widow maker” ECG patterns:
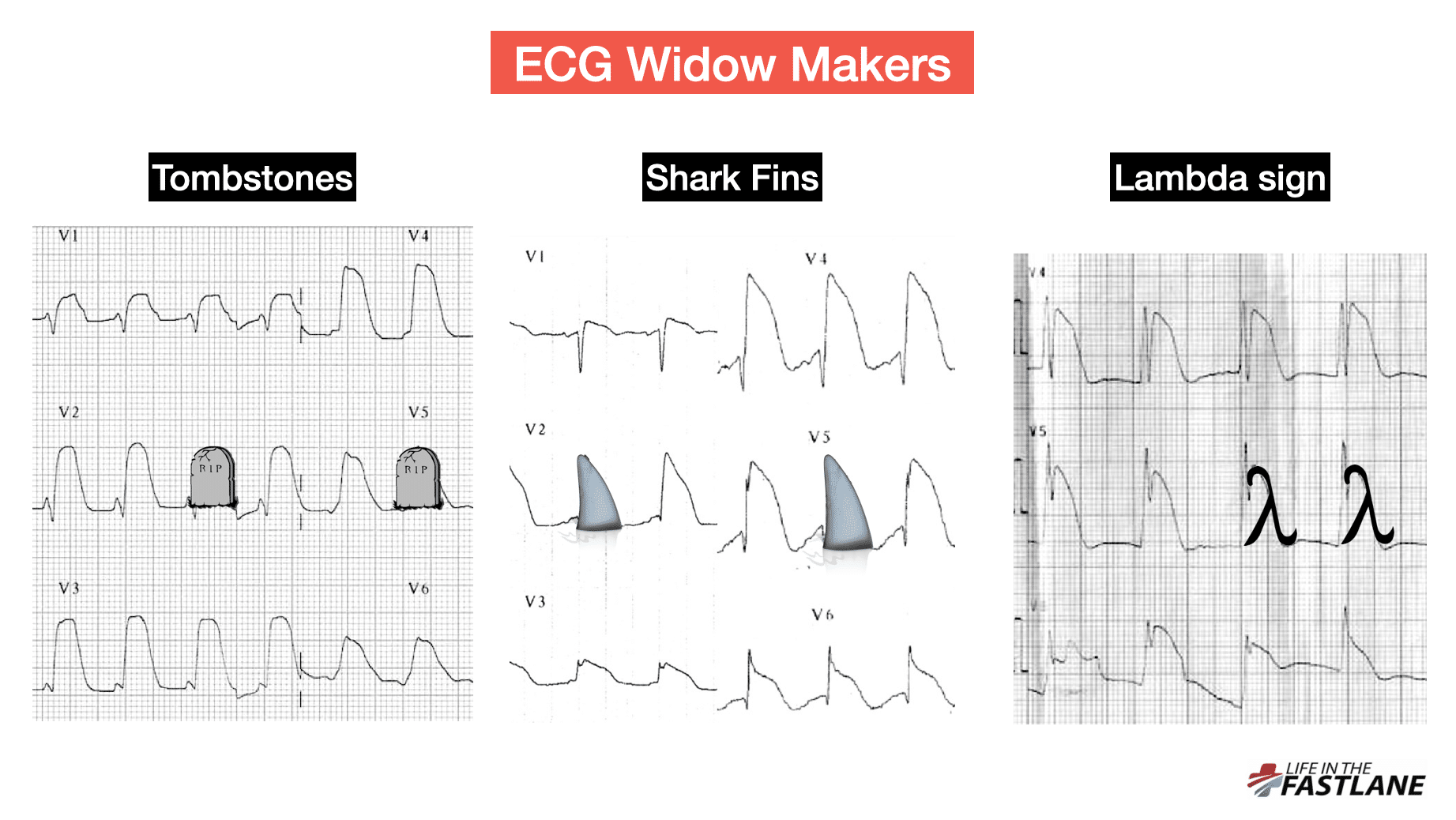
Massive ST elevation often merges with hyperacute T waves in these patterns creating the appearance of a broad QRS complex – this can be mistaken for hyperkalaemia or a broad complex tachycardia.
Patients with any three of these “widow maker” patterns are at extremely high risk of lethal ventricular arrhythmias. Check out this great case discussion by Dr Sam Ghali and Dr Stephen Smith of a 100% RCA occlusion presenting with shark fin ST elevation morphology.
- Ghali S, Smith S. “Shark Fin”: A Deadly ECG Sign that you Must Know! Dr Smith’s ECG Blog
References
Further Reading
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
TOP 100 ECG Series
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.
