
![]()
ECG Case 036
Middle-aged patient presenting with chest pain. Describe the ECG.
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
Main Abnormalities
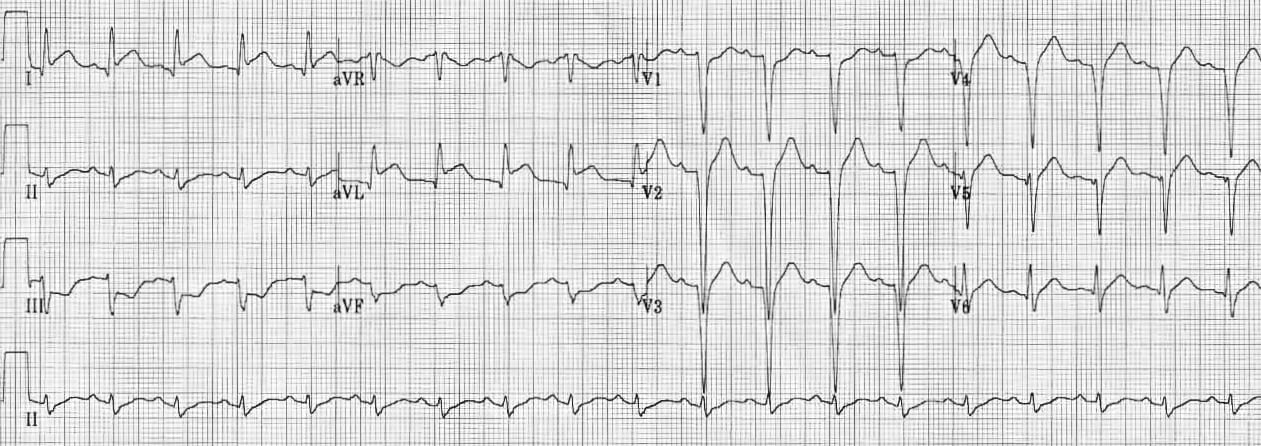
This ECG is a good example of high lateral STEMI:
- ST elevation is confined primarily to the high lateral leads I and aVL
- There is reciprocal ST depression in the inferior leads II, III and aVF
- The deep Q waves and poor R wave progression in V1-4 suggest prior anteroseptal infarction or dilated cardiomyopathy
High lateral STEMI is classically associated with occlusion of the first diagonal branch (D1) of the LAD, but may also occur with occlusion of the obtuse marginal branch (OM) of the circumflex artery, or the ramus intermedius.
CLINICAL PEARLS
High lateral STEMI may be extremely subtle. Sometimes the only clue is the presence of new inferior ST depression. Such localised ST depression should always be considered to be reciprocal change rather than “inferior ischaemia” as ST depression does not localise.
References
Further Reading
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
TOP 100 ECG Series
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.
