
![]()
Second-degree Atrioventricular block
Eponymythology: The myths behind the history
Second degree AV block
We review the early development of arrhythmia recording and the contributions of Luciani, Galabin, Gaskell, Wenckebach, Hay and Mobitz to the current terminology associated with the categorization of Second-degree Atrioventricular block
ECG patterns that describe the behavior of the PR intervals (in sinus rhythm) in sequences with at least 2 consecutively conducted PR intervals in which a single P wave fails to conduct to the ventricles
Mobitz Type I (Wenckebach AV block)
- Progressive prolongation of the PR interval culminating in a non-conducted P wave
- PR interval is longest immediately before the dropped beat
- PR interval is shortest immediately after the dropped beat

Mobitz Type II (Hay AV block)
- Intermittent non-conducted P waves without progressive prolongation of the PR interval
- PR interval in the conducted beats remains constant.
- P waves ‘march through’ at a constant rate.
- RR interval surrounding the dropped beat(s) is an exact multiple of the preceding RR interval (e.g. double the preceding RR interval for a single dropped beat, treble for two dropped beats, etc).

Arrows indicated ‘dropped’ QRS complexes (i.e. non-conducted P waves). Type I and Type II describes the ‘ECG pattern’ and the anatomical site of the block should not be inferred by this
History of Second-degree Atrioventricular block
1873 – Luigi Luciani demonstrated cardiac group beating which he named ‘periodic rhythm’ whilst studying frogs’ hearts in Carl Ludwig’s laboratory in Leipzig. Luciani used a tonographic apparatus for the graphic representation of the ventricular pulse of the frog heart preparation [1873;25:11–94]
Luciani frog heart ventricular pulse experiments
Luciani Periods (Right to left) 1873

Periodic ventricular rhythm shown by frog heart tied at atria 2mm above AV groove, filled with rabbit serum, and attached to tonographic apparatus – Luciani 1873
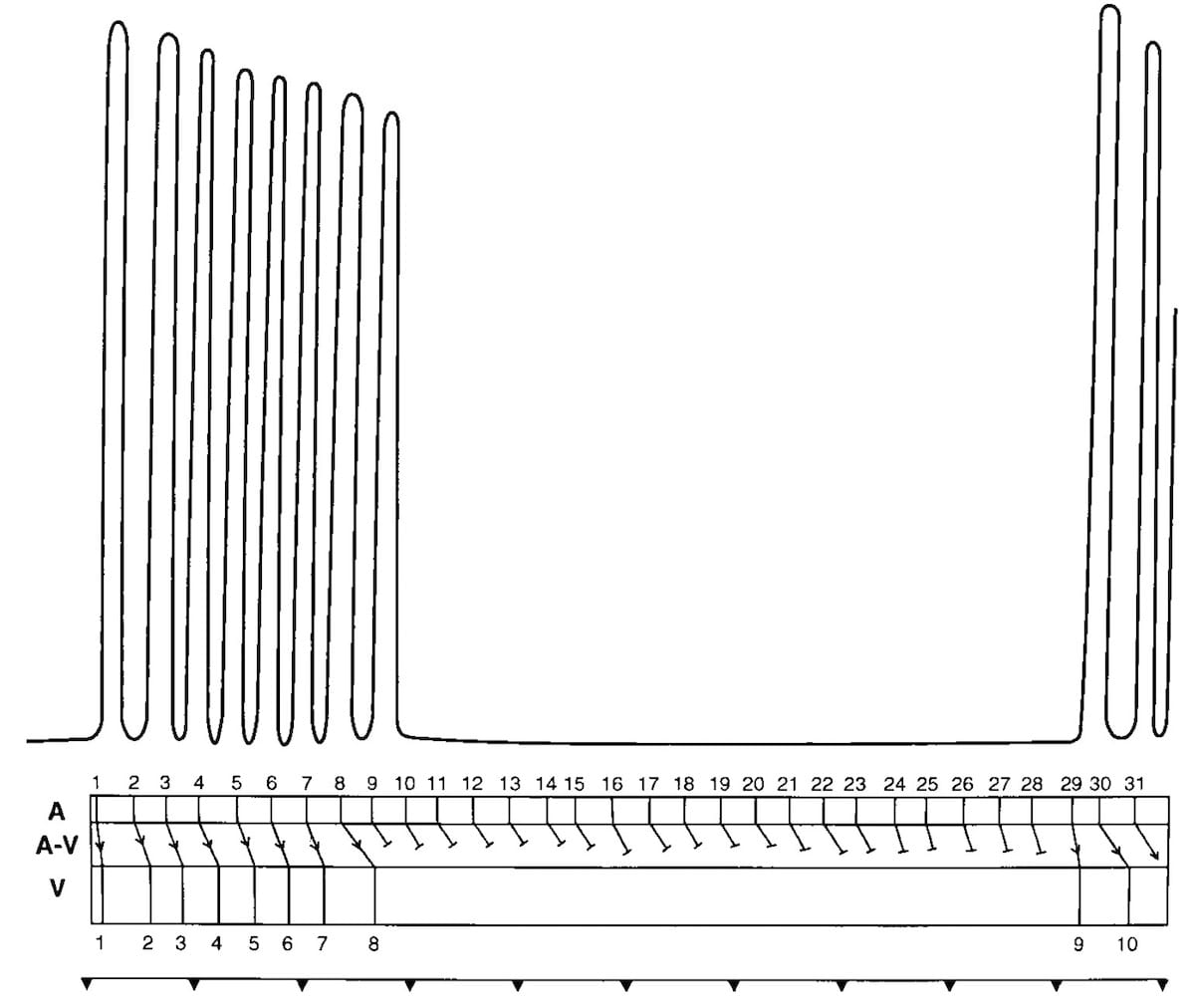
Ventricular pulse waves of Luciani groupings (with pause) taken from the original figures and enlarged 8x. Upshaw and Silverman created a laddergram (drawn beneath the waves) which illustrates Wenckebach second-degree AV block. Circulation. 2000;101:2662-2668
1875 – Alfred Galabin was the first to demonstrate atrioventricular block in humans. He used the apexcardiogram to study patients with mitral stenosis and found a patient (Richard B-) with a slow pulse; the case report in which he described atrial contraction asynchronous with ventricular contraction. [1875;20:261–314]
Subsequent analysis of Galabin’s studies suggest his patient had advanced AV block with 3-to-1 and 2-to-1 AV conduction with Wenckebach periodicity
Galabin Apexcardiogram of Richard B-
Richard B-, was a 34 year old male who presented with a pulse of 25-30 bpm. Figure 14 (XIV) demonstrates ‘wavy movements‘ in the long diastolic interval and could be attributed to movement artefact. However a repeat study taken later in the same day, figure 15 (XV), demonstrates an almost exact repetition.
Galabin postulated that the atria of the heart contracted twice in the interval between two ventricular contractions, and sometimes singly in the midst of a long pause instead of just before the systole of the ventricle.

1898 – Karel Frederik Wenckebach (1864-1940) consulted a 40-year-old woman with an irregular pulse which he interrogated using a sphygmogram and tuning fork. He noted there were regular pauses every 3 to 4 beats, but the small extra pulse seen during pauses were longer, and subsequent intervals were smaller. The first interval after each pause was longer, and subsequent intervals were shorter.
1899 – Wenckebach credited Luciani as the first to describe this recurrent pattern in his 1873 frog heart experiments and defined this form of group beating as ‘Luciani’schen Perioden’ (Luciani periods)
Original
English
Man spricht in diesen Fällen von einer “periodischen Function” des Herzens; die Gruppen werden nach dem Entdecker “Luciani’sche Perioden” genannt.…es sich hier um eine regelmässige Herzthätigkeit handelt, welche von einem constantcn schädlichen Einfluss gestört wird. Dieser Einfluss ist ein negativ dromotroper Einfluss, wie aus einer sorgfältigen Vergleichung dieses Pulses mit der Ventrikelthätigkeit des in Luciani’schen Perioden klopfenden Froschherzens hervorgeht.
In these cases one speaks of a “periodic function” of the heart; the groups are called “Luciani periods” after the discoverer… it is a regular cardiac activity, which is disturbed by a constant harmful influence. This influence is a negative dromotropic influence, as can be seen from a careful comparison of this pulse with the ventricular activity of the frog heart pounding in Luciani’s periods.
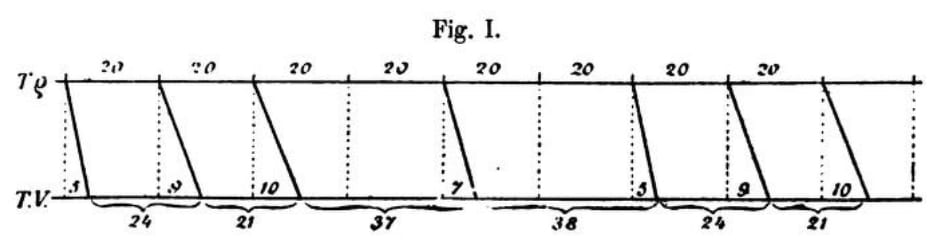
Wenckebach’s figure demonstrates a constant atrial rate (top line) with diagonal lines (representing AV conduction) progressively lengthening before a beat being missed/dropped. This is followed by the recommencement of the cycle.
With the advent of electrocardiography in the early 20th century, this form of group beating became known as ‘Wenckebach periodicity‘ and later as ‘Mobitz type I atrioventricular block‘.
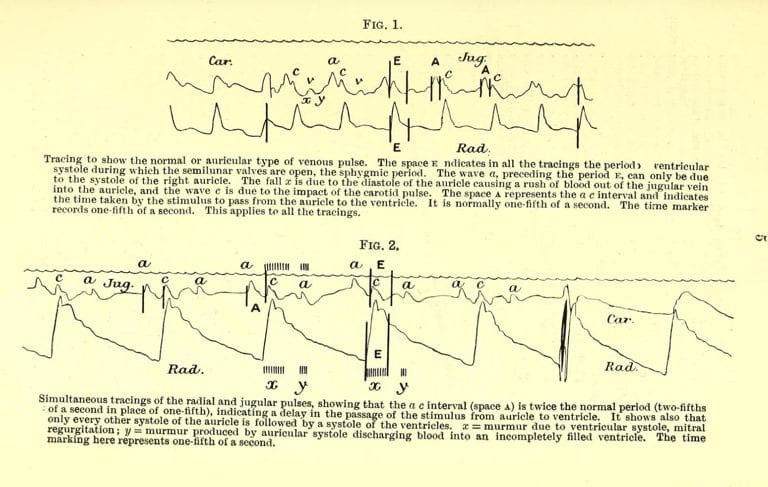
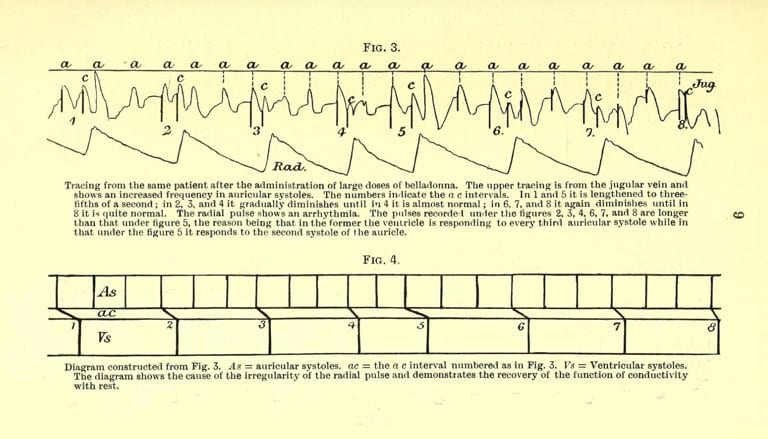
1906 – John Hay (1873–1959) kymographically recorded simultaneous jugular venous and radial arterial pulses of a 65-year-old man with a slow pulse. He observed that the a-to-c intervals of the jugular venous waves remained constant until an a (jugular venous) wave occurred that was not followed by the c (radial pulse) wave. The pause was equal to 2 atrial pulse-wave intervals [1906; 167(4299): 139-143]
1906 – Wenckebach ** acknowledged Hay’s report, and suggested that the pauses found in Hay’s patient were the result of both abnormal AV conduction and abnormal ventricular excitability. [Archiv für Physiologie 1906:332]
**Hay had also spent six month’s studying with Wenckebach at Freiburg.
1924 – Woldemar Mobitz (1889–1951) applied a mathematical approach to analyzing arrhythmias by graphing the relationship of changing atrial rates and premature beats to AV conduction
He classified second-degree atrioventricular (AV) block into 2 principle types, subsequently referred to as Mobitz type I (Wenckebach) and Mobitz type II (Hay). [1924;41:180-237]
Mobitz Type I (Wenckebach)
The top line of the laddergram demonstrates the time between atrial contraction (equivalent to P-P intervals) to be constant.
The middle diagonal line depicts AV conduction (P-R interval), which gradually lengthens until the point at which AV conduction is absent altogether. After this point, the cycle starts again.
The bottom line of the laddergram illustrates increasing time periods between ventricular contraction (R-R interval), before a long pause as a result of the dropped beat, followed by a repeat of the cycle.
Effectively a 6:5 Type I block.

Mobitz Type II (Hay)
Atrial rate is constant, AV conduction rates are constant when successful, and ventricular contraction is present only after successful AV conduction.

The rate of ventricular contraction is the same as rate of atrial contraction, or where AV block occurs, is an exact multiple of the atrial rate, as below algebraically
Type II AV Block: Laddergram – Mobitz 1924.

Associated Persons
- Luigi Luciani (1840–1919)
- Alfred Lewis Galabin (1843–1913)
- Walter Holbrook Gaskell (1847-1914)
- Karel Frederik Wenckebach (1864–1940)
- John Hay (1873–1959)
- Woldemar Mobitz (1889–1951)
Alternative names
- Mobitz Type I – Luciani periods, Wenckebach Periodicity, Wenckebach AV block
- Mobitz Type II – Hay AV block
Controversies
An apparent and remarkable absence of controversy, with frequent acknowledgement of the work of both their preceding and contemporary colleagues.
Despite a well defined historical timeline only the names of Wenckebach and Mobitz remain in common use
LITFL Related Links
- AV Block: 2nd degree, Mobitz I
- AV Block: 2nd degree, Mobitz II.
- AV block: 2nd degree, “fixed ratio” blocks.
- AV block: 2nd degree, “high-grade” AV block
- Medical Eponym Library – A-Z of eponymous medical pioneers
References
- Luciani L. Eine periodische Function des isolirten Froschherzens [A periodic function of the isolated frog heart]. Berichte über die Verhandlungen der Königlich Sächsischen Gesellschaft der Wissenschaften zu Leipzig. 1873;25:11–94.
- Galabin AL. On the interpretation of cardiographic tracings, and the evidence which they afford as to the causation of the murmurs attendant upon mitral stenosis. Guy’s Hosp Rep 1875;20:261–314.
- Wenckebach KF. Zur Analyse des unregelmässigen Pulses [On the analysis of irregular pulses] Zeitschrift Für Klinische Medizin. [I 1899; 36: 181-199] [II 1899; 37: 475–488] [III 1900; 39: 293-305] [IV 1902: 44: 218-225]
- Hay J. Bradycardia and cardiac arrhythmia produced by depression of certain of the functions of the heart. Lancet 1906;167(4299):139-143
- Wenckebach KF. Beiträge zur Kenntnis der menschlichen Herztätigkeit [Contributions to the knowledge of human cardiac activity]. Archiv für Anatomie und Physiologie. I 1906:297–354. II 1907:1-24
- Mobitz W. Über die unvollständige Störung der Erregungs-überleitung zwischen Vorhof und Kammer des menschlichen Herzens. [On the partial block of impulse conduction between atrium and ventricle of human hearts] Zeitschrift Fur Die Gesamte Experimentelle Medizin. 1924;41:180-237
- Upshaw CB Jr, Silverman ME. Luigi Luciani and the earliest graphic demonstration of Wenckebach periodicity. Circulation. 2000; 101(22): 2662-8.
- Upshaw CB Jr, Silverman ME. Alfred Lewis Galabin and the first human documentation of atrioventricular block. Am J Cardiol. 2001; 88(5): 547-50.
- Silverman ME, Upshaw CB Jr. Walter Gaskell and the understanding of atrioventricular conduction and block. J Am Coll Cardiol. 2002; 39(10): 1574-80.
- Silverman ME, Upshaw CB Jr, Lange HW. Woldemar Mobitz and His 1924 Classification of Second-Degree Atrioventricular Block. Circulation. 2004; 110(9): 1162-1167
eponymictionary
the names behind the name