
![]()
Spodick sign
Downsloping TP segment seen as an early ECG manifestation in ~30% of patients with pericarditis, best visualised in leads II and the lateral precordial leads
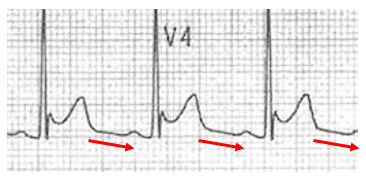
ECG changes associated with Stage I pericarditis, first described by David H. Spodick in 1974. The sign remained relatively unevaluated until a recent retrospective analysis in 2020. Witting et al, considered an ECG to demonstrate Spodick’s sign when at least two leads had TP downsloping of at least 1 mm.
Clinical significance
- Potential useful distinguishing ECG feature between acute pericarditis and ACS
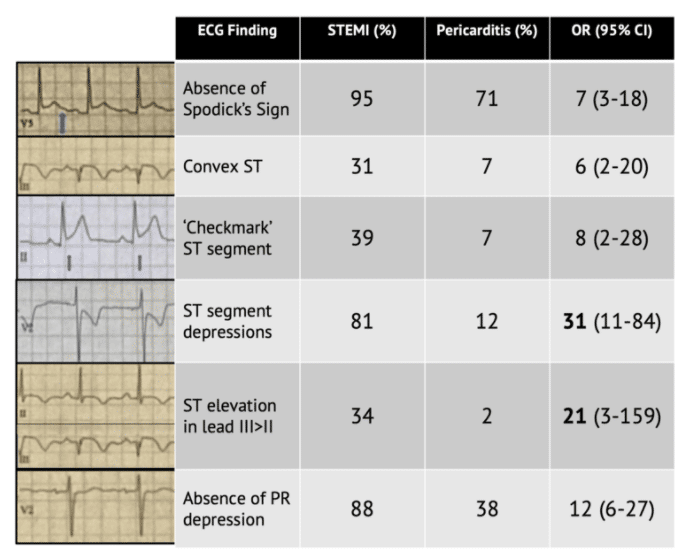
- Witting found that Spodick’s sign occurred in 29% of patients with pericarditis and 5% of patients with STEMI (OR 5.9)
- PR depression alone can be a masquerader as it is seen in 12% of patients with STEMI
- A separate prospective study by Porela et al found that PR depression had a high sensitivity (88%) for myopericarditis but a low specificity
In 1973 and 1974, Spodick described the classic four-stage evolution of electrocardiographic changes with pericarditis, including ST elevations and PR depressions.
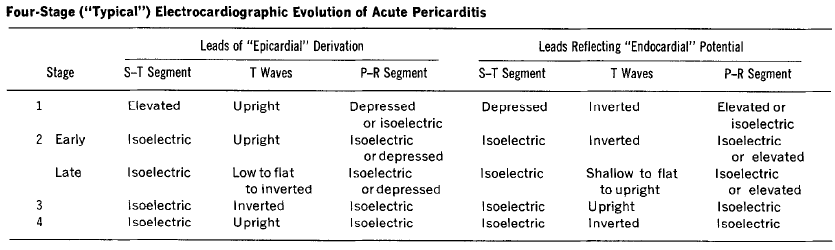
Note: Less than 50% of patients progress through all four classical stages and evolution of changes may not follow this typical pattern
Spodick specifically described downsloping of the T-P segment, alter termed the Spodick sign
…the electrocardiographic registration of atrial injury in acute pericarditis is analogous to that of the stage 1 ventricular subepicardial injury in that each follows the orientation of its respective normal recovery (T) wave.
Since most atrial tissue lies posteriorly, to the right, and relatively cephalad of the ventricles, the orientation of a vector of generalized atrial injury (AP-R) would be expected to be to the right and superior (as shown by the frontal plane AP) and also posterior. The predominant P-R segment depressions across the precordium document the posterior component.
Because of these P-R segment deviations, it is of practical importance in acute pericarditis to consider the T-P segment to be the electrocardiographic base line to avoid mistaking P-R segment depression for S-T segment elevation.
Spodick 1974
Differentiating STEMI from pericarditis
The most discriminating features remain as ST depression, ST elevation in lead III >II, and absence of PR depression. It is thus still recommended to look for features of STEMI first on the ECG with ST elevation:
- Search for ST depression (aside from leads aVR and V1)
- Look for ST elevation in III > II
- Search for horizontal or convex upward ST elevation
Following this, additional features such as Spodick’s sign can be reviewed to further differentiate the diagnosis of pericarditis.
Examples
Example 1
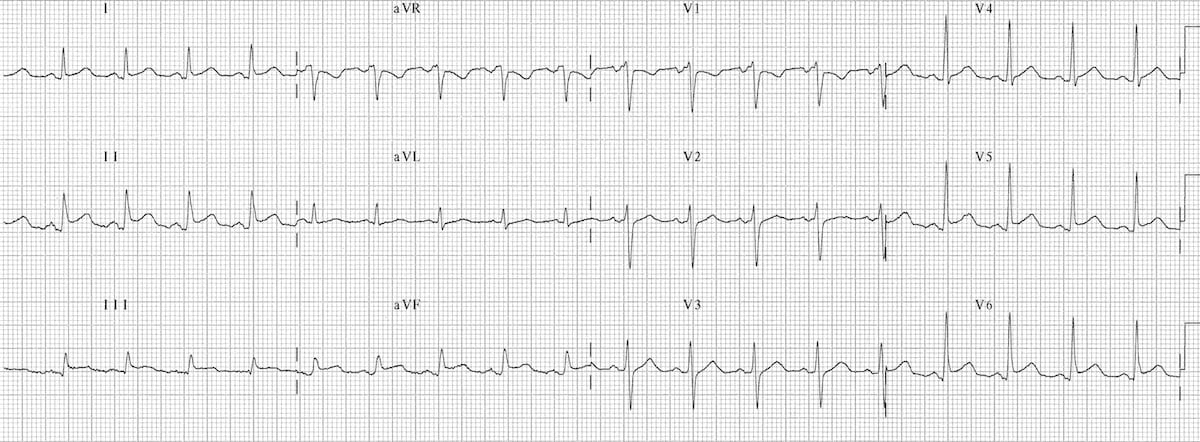
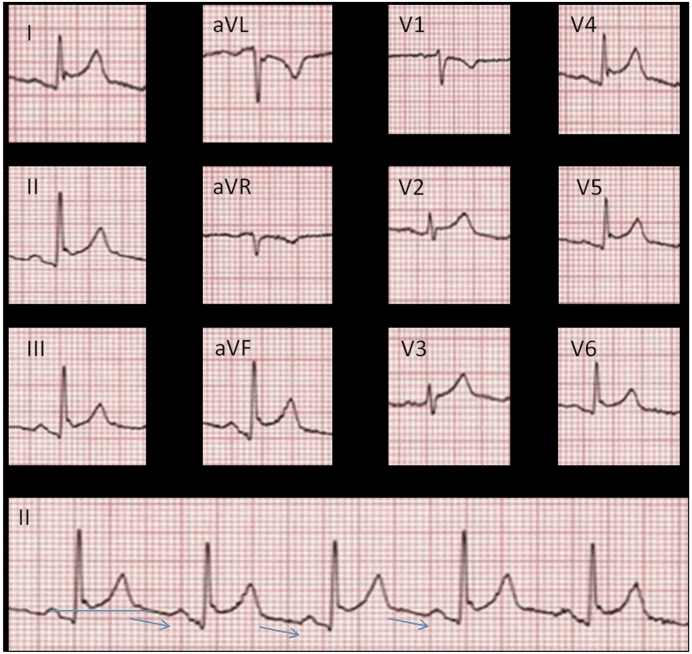
Acute pericarditis:
- Sinus tachycardia
- Widespread concave STE and PR depression (I, II, III, aVF, V4-6).
- Reciprocal ST depression and PR elevation in V1 and aVR
- Spodick’s sign best visualised in lead II
Example 2

Example 3

Associated Persons
- David H Spodick (1927-2019)
ECG Library
- Burns E. Pericarditis. LITFL ECG Library
- Burns E. The ST Segment. LITFL ECG Library
References
- Spodick DH. Diagnostic electrocardiographic sequences in acute pericarditis. Significance of PR segment and PR vector changes. Circulation. 1973 Sep;48(3):575-80.
- Spodick DH. Electrocardiogram in acute pericarditis. Distributions of morphologic and axial changes by stages. Am J Cardiol. 1974 Apr;33(4):470-4.
- Ginzton LE, Laks MM. The differential diagnosis of acute pericarditis from the normal variant: new electrocardiographic criteria. Circulation. 1982 May;65(5):1004-9.
- Makaryus JN, Makaryus AN, Boal B. Spodick’s sign. Am J Med. 2008 Aug;121(8):693-4.
- Makaryus JN et al. Diagnostic issues in the clinical management of pericarditis. Int J Clin Pract. 2010 Sep;64(10):1384-92.
- Chhabra L, Spodick DH. Ideal isoelectric reference segment in pericarditis: a suggested approach to a commonly prevailing clinical misconception. Cardiology. 2012;122(4):210-2.
- Maeba H. Isoelectric reference for pericarditis: TP may be better than PR. Cardiology. 2012;123(1):39-40
- Masek KP, Levis JT. ECG Diagnosis: Acute Pericarditis. Perm J. 2013 Fall; 17(4): e146.
- Chaubey VK. Spodick’s Sign: A Helpful Electrocardiographic Clue to the Diagnosis of Acute Pericarditis. Perm J. 2014 Winter; 18(1): e122.
- Smith SW. Diffuse ST Elevation and Chest Pain, What is it? 6 July 2015 Dr. Smith’s ECG Blog
- Witting MD et al. Evaluation of Spodick’s Sign and Other Electrocardiographic Findings as Indicators of STEMI and Pericarditis. J Emerg Med. 2020 Mar 25. pii: S0736-4679(20)30020-2.
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
ECG LIBRARY
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |
