
![]()
Abdominal CT: Cancer staging
Differentiating between phases of the CT exam
Many cancer staging studies are performed with a single portal venous phase examination. However, there are several cancers that require multiphasic exams, where images are obtained at different time points after IV contrast is given.
Screening and staging of the following cancers involve special multiphasic CT exams:
Pancreas adenocarcinoma
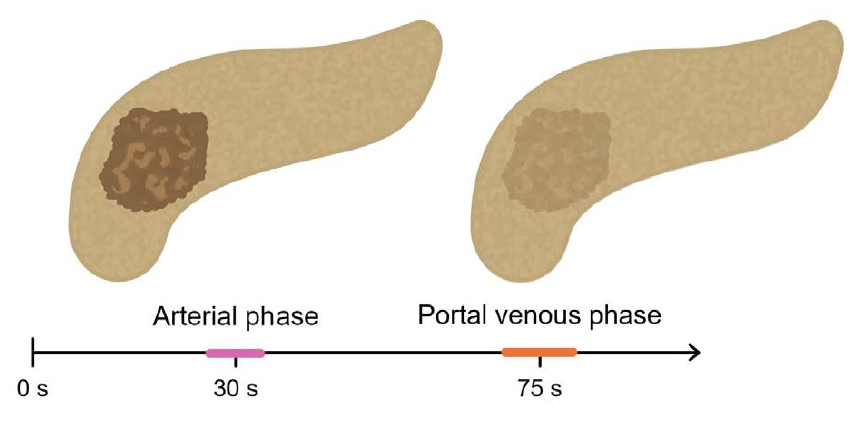
Staging pancreas adenocarcinoma requires both late arterial and portal venous phase imaging.
The late arterial phase is most often the best phase to see a mass in the pancreas. At this time point, the mass will usually enhance less, appearing darker than the surrounding pancreatic tissue. In the portal venous phase, the mass often blends in with the rest of the pancreas and can be difficult to see.
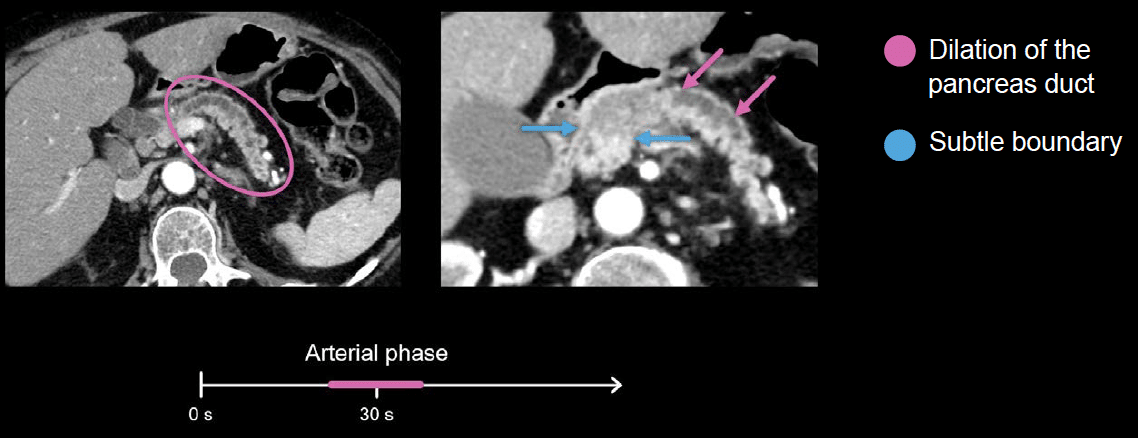
Often, the first CT finding to raise concern about a pancreas mass is dilation of the pancreas duct. Normally the duct is barely visible, so if you can see it, you are right to suspect a mass causing an obstruction.
When we zoom in on the image below, we are able to see a relatively subtle boundary between the pancreas tissue and the mass, which has decreased enhancement. On the other side, the dilated duct leads right into the mass, helping to identify the boundary
In many pancreas adenocarcinoma cases, the primary tumor can be difficult to see. The best way to determine its boundaries is to look for the point where the common bile duct or the pancreas duct change size due to obstruction caused by the tumour
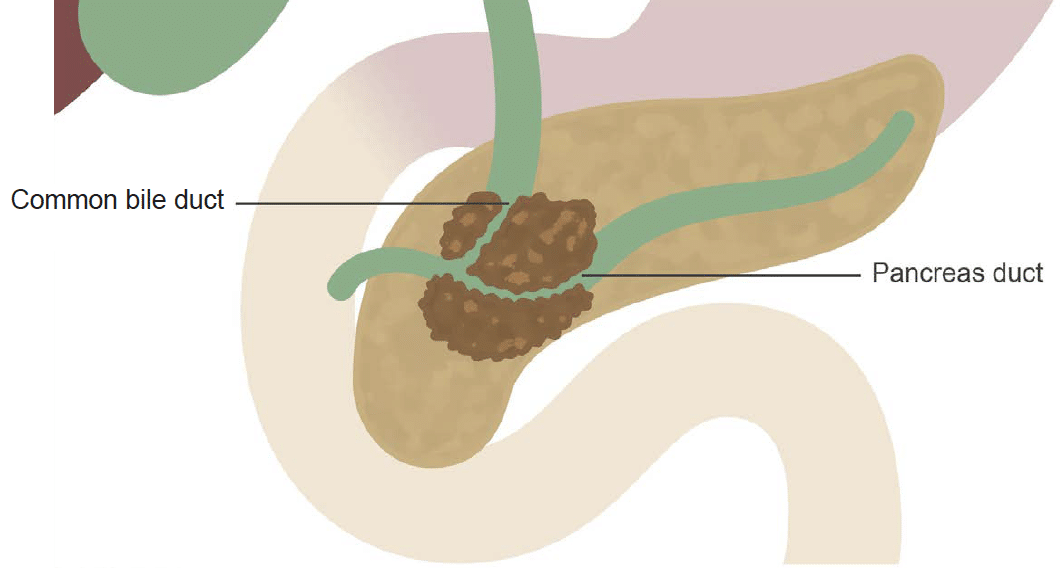
In the images below, both the common bile duct and the pancreas duct are obstructed by a pancreas head adenocarcinoma, referred to as the double duct sign. Although we cannot see the primary tumour well, we can infer its boundaries by the location of the abrupt tapering of these ducts.

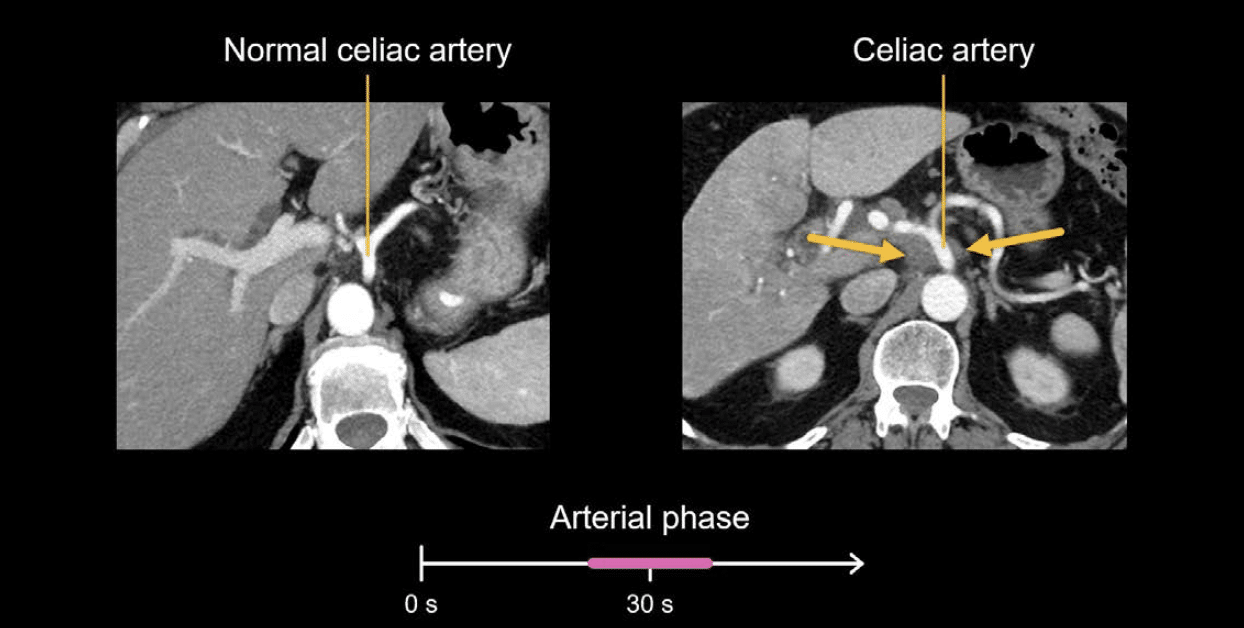
A major part of local staging of pancreas adenocarcinoma is to look for vascular involvement, both arterial and venous. Pancreas adenocarcinoma often spreads locally along the vasculature. To look for vascular involvement, we carefully review all vascular structures in the late arterial and portal venous phases for:
- subtle soft tissue thickening
- stranding
- narrowing
In the example below on the right, we can see soft tissue thickening encasing the coeliac artery when compared to the normal coeliac artery on the left.
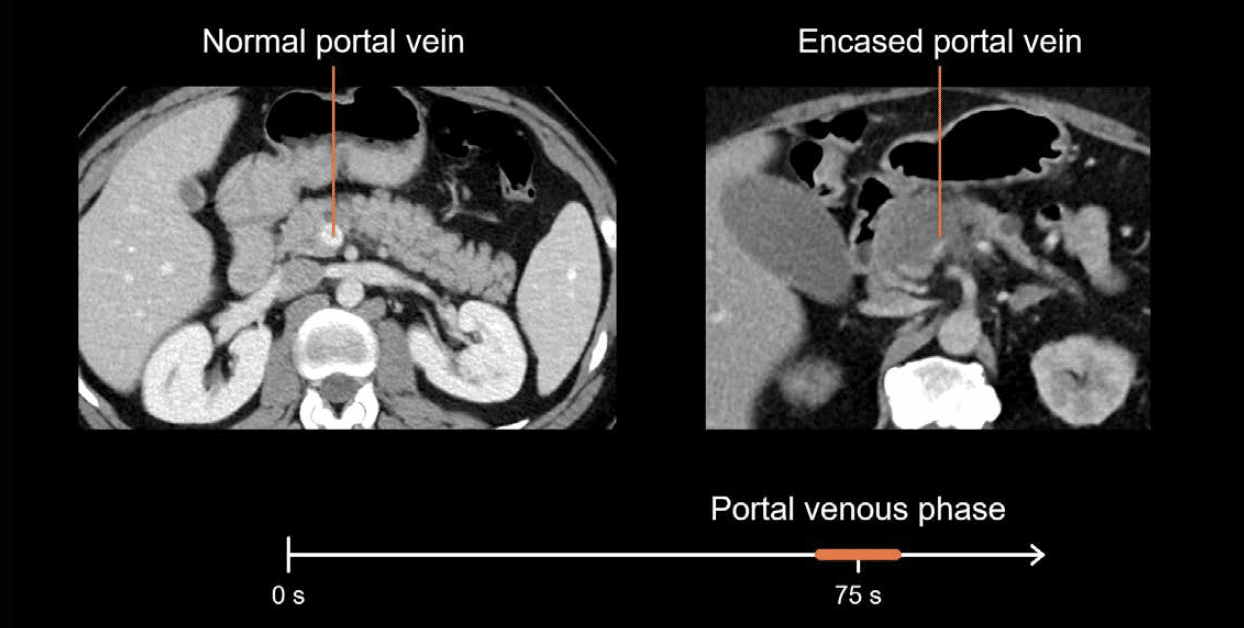
Similarly, below we can compare a normal rounded portal vein near the pancreas head to the narrowed, slit-like portal vein seen in the image on the right. This appearance indicates venous encasement and narrowing by the pancreas head mass.
Metastases and abnormal lymph nodes
The portal venous phase is also used to complete staging of cancers in the abdomen and pelvis, which includes looking for metastases and abnormal lymph nodes. Metastases are sites in the body where tumour cells have spread and are separate from the primary, or original, site of the tumour. These sites can include the organs, lymph nodes, bones, and bowel.
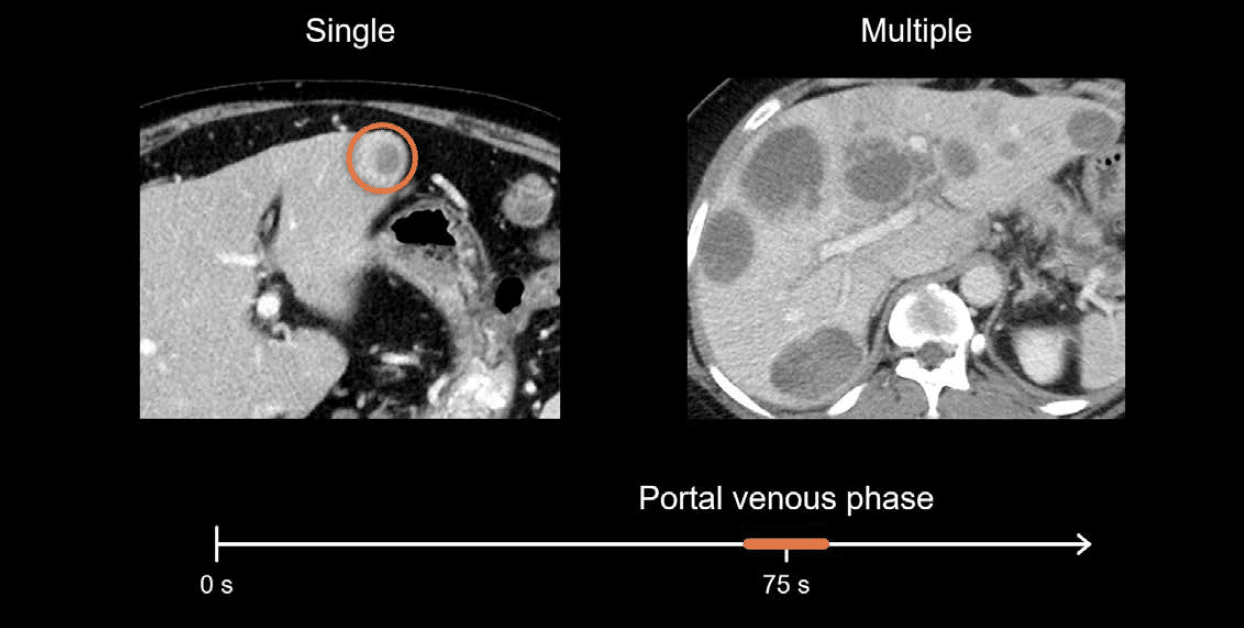
A common site for cancer to spread is the liver. The two examples below show the typical appearance of single and multiple liver metastases, which are generally rounded masses that enhance less than the background liver.
Neuroendocrine tumour and renal cell carcinoma
Both neuroendocrine tumours and renal cell carcinomas (RCC) are known to produce hypervascular metastases, most commonly in the liver.
These liver metastases appear bright on the late arterial phase images, but can frequently blend in during the portal venous phase. Because of this characteristic, you can use multiphasic CT for staging these cancers.
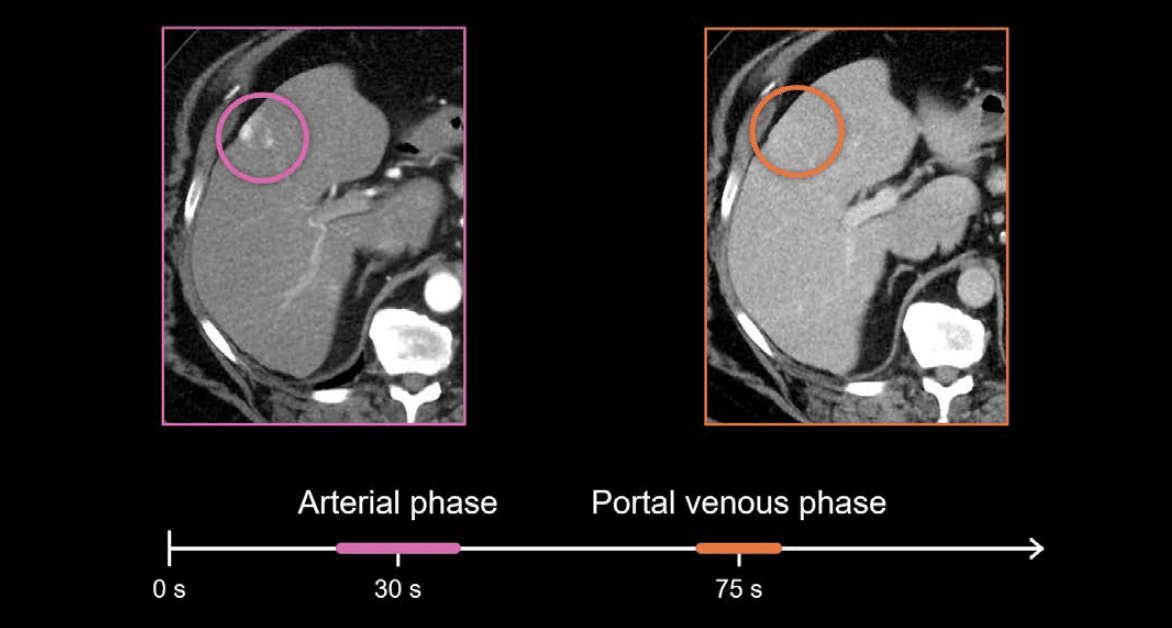
Example 1: RCC staging
Renal cell carcinoma staging exam, the liver metastasis is clearly visible on the arterial phase image but is nearly impossible to locate on the portal venous phase image.
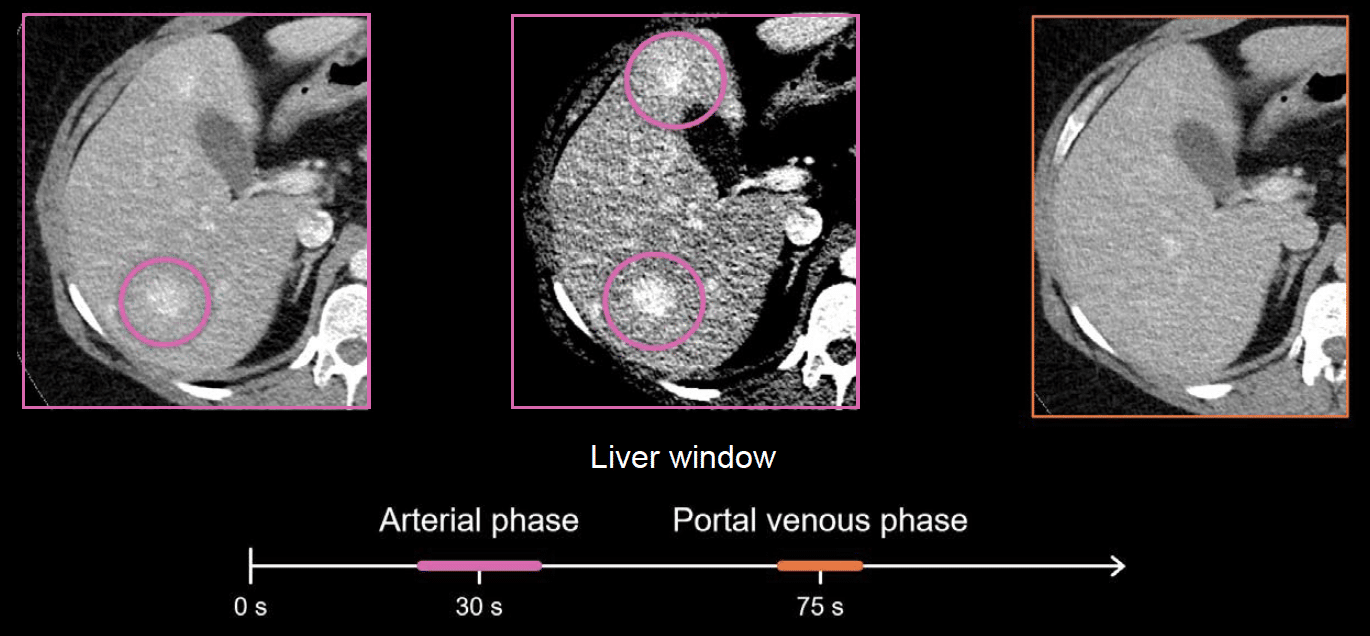
Example 2: liver metastasis from a gastric neuroendocrine tumour
The liver mass is well defined and easy to see in the arterial phase image – it really jumps out, and we can see an additional mass when the liver window is applied. However, both masses are nearly impossible to see on the portal venous phase image.
For this reason, both neuroendocrine tumours and renal cell carcinomas benefit from a dual-phase examination which includes both arterial and portal venous phase imaging.
Hepatocellular carcinoma (HCC)
Hepatocellular carcinoma (HCC) is another cancer that requires multiphasic imaging. However, unlike other cancers, HCC can be diagnosed based on imaging features alone, in many cases.
Arterial enhancement
The liver receives most of its blood supply from the portal vein. HCC, on the other hand, gets most of its blood supply from the hepatic artery.
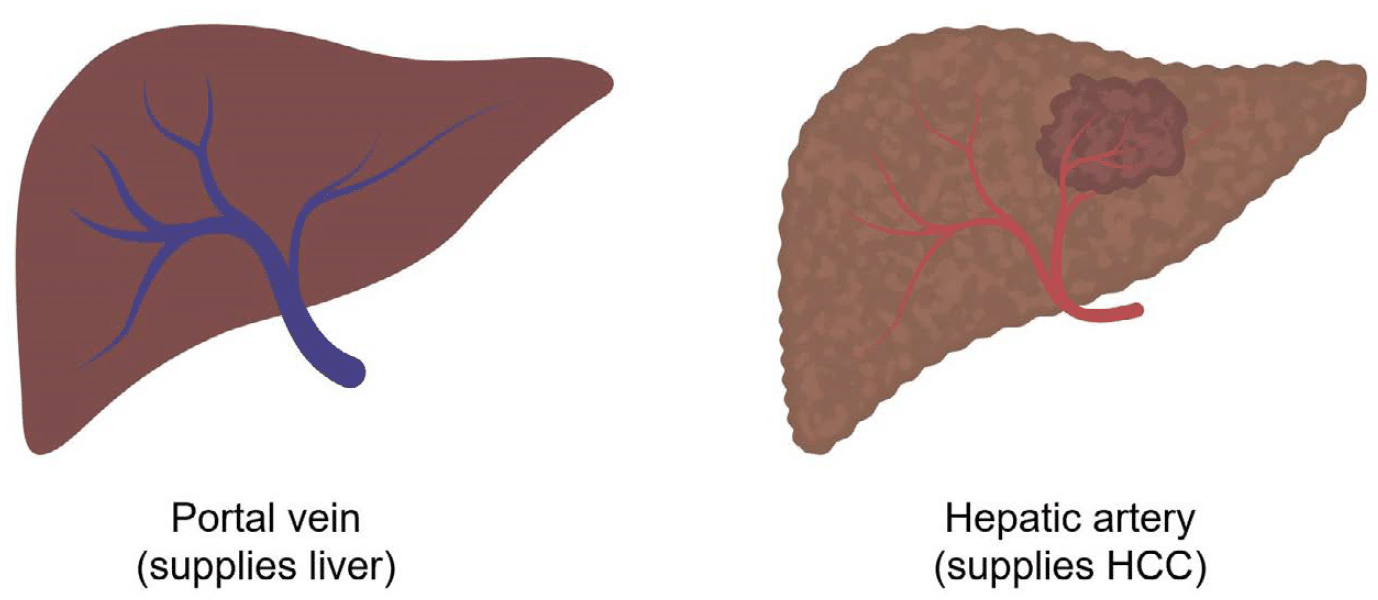
This means that the HCC will have more arterial phase enhancement from the hepatic artery when compared to the rest of the liver since the normal liver tissue is getting more blood supply from the portal system.
Conversely, the HCC will look darker than the rest of the liver during the portal venous phase, because at this point, the liver has received contrast-mixed blood from the portal vein and the arterial flow in the HCC has washed out.
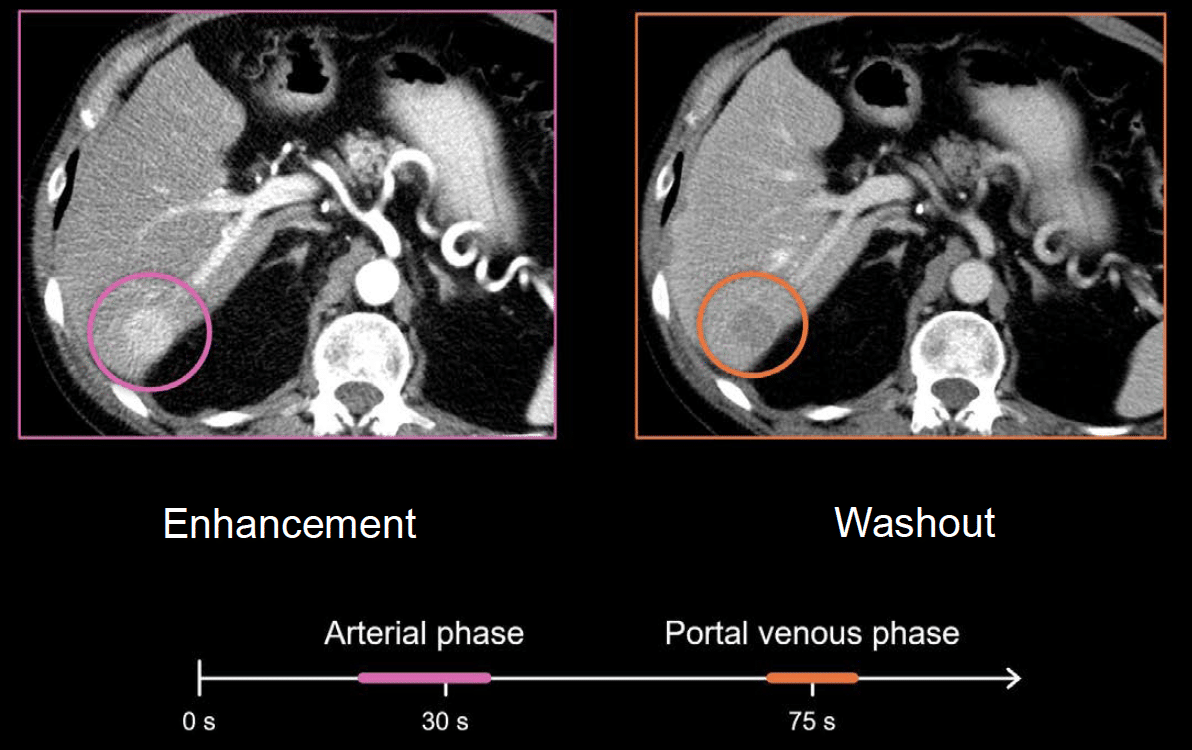
Washout
So, when looking at the liver using arterial phase imaging, an HCC will often appear as a rounded mass that is enhancing more (i.e. brighter) compared to the background liver. In comparison, during portal venous and other delayed phases, the HCC will enhance less (i.e. washout) compared to the background liver.
Enhancing capsule
Another feature that’s important for diagnosing HCC is something called an enhancing capsule, which is a thin bright rim around the tumour that can be seen on the portal venous or delayed phases. While it’s important to look for, it can be hard to see on CT and is often better seen on MRI.

Example 3: arterial hyperenhancement.
Let’s look at another example of HCC where we are interested in characterising a rounded mass in the right hepatic lobe. In this case, the mass is brighter than the rest of the liver during the arterial phase image. This is called arterial hyperenhancement.

On the portal venous phase image, the mass is fainter—it enhances less, and it starts to blend in with the rest of the liver. However, on the delayed phase image (taken between 120–180 seconds after IV contrast is given), the washout becomes more apparent. Notice how much darker the mass is compared to the rest of the liver, and it even has a thin bright rim, or enhancing capsule, surrounding it.
Therefore, when diagnosing HCC, arterial phase, portal venous phase, and delayed phase provide essential information about arterial enhancement, washout, and an enhancing capsule, which enables us to make the diagnosis with confidence.
This is an edited excerpt from the Medmastery course Abdominal CT Essentials by Michael P. Hartung, MD. Acknowledgement and attribution to Medmastery for providing course transcripts.
- Hartung MP. Abdominal CT: Common Pathologies. Medmastery
- Hartung MP. Abdominal CT: Essentials. Medmastery
- Hartung MP. Abdomen CT: Trauma. Medmastery
References
- Top 100 CT scan quiz. LITFL
Radiology Library: Abdominal CT Basics
- Hartung MP. Abdominal CT: Phases. LITFL
- Hartung MP. Abdominal CT: Cancer staging. LITFL
- Hartung MP. Abdominal CT: GU imaging. LITFL
- Hartung MP. Abdominal CT: Urogram. LITFL
- Hartung MP. Abdominal CT: Cystogram. LITFL
- Hartung MP. Abdominal CT: Flank pain imaging. LITFL
Abdominal CT interpretation

Assistant Professor of Abdominal Imaging and Intervention at the University of Wisconsin Madison School of Medicine and Public Health. Interests include resident and medical student education, incorporating the latest technology for teaching radiology. I am also active as a volunteer teleradiologist for hospitals in Peru and Kenya. | Medmastery | Radiopaedia | Website | Twitter | LinkedIn | Scopus

MBChB (hons), BMedSci - University of Edinburgh. Living the good life in emergency medicine down under. Interested in medical imaging and physiology. Love hiking, cycling and the great outdoors.
