
![]()
Abdominal CT: Phases
Differentiating between phases of the CT exam
To make sense of CT exams, we need to understand what happens after we inject IV contrast and how it results in tailored CT examinations. CT exams can be divided into phases that can be shown on a timeline.
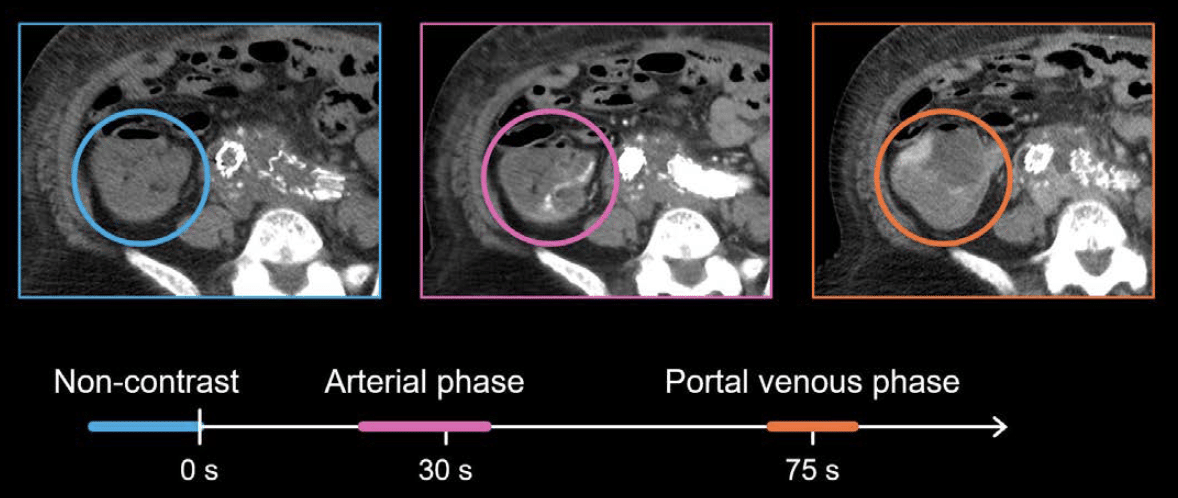
The exam starts by giving IV contrast (shown at zero seconds) and can span over more than eight minutes. The three common phases are:
- Zero point (before contrast)
- Arterial phase
- Portal venous phase
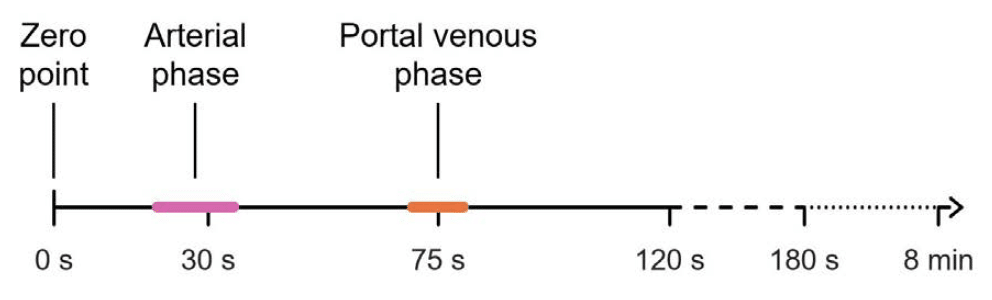
All three of these phases occur within the first 1.5 minutes of the exam. The different phases simply refer to how quickly the CT is performed after the contrast is injected intravenously. Different structures are best evaluated at each time point.
Portal venous phase
The most common time point in abdominal CT is the portal venous phase, which is obtained around 70–80 seconds after contrast is injected. This phase provides the best balance of solid organ, bowel, and vascular enhancement for general imaging as we can see from the axial and coronal images

Arterial phase
The arterial phase is the second most common sequence to obtain and can range from 20–35 seconds after contrast injection. The exact timing depends on whether you want to evaluate the vessels or check the organs for abnormalities, such as tumors with a rich arterial blood supply.
As you can see in the following images, the aorta is really bright in the image on the left. We know we are in the early arterial phase because the liver and the spleen still appear dull and grey. In the later portal venous phase (shown in the image on the right), you will notice that the aorta looks less bright compared to the earlier arterial phase, but you can see the liver and spleen better because more contrast-mixed blood has entered those organs by the 75-second time point.

Multiphasic exams in emergency settings
While the standard portal venous phase is the go-to exam for abdominal imaging, there are times when your patient will benefit from a multiphasic specialty examination. In multiphasic exams, images are obtained at several different time points, both before and after IV contrast is injected in the patient, rather than just in the portal venous phase.

Example 1: Mesenteric ischaemia
Mesenteric ischaemia is caused by a blockage of the arteries or veins that serve the bowel, and it is a common reason for multiphasic CT. Typically, the patient will present with severe abdominal pain, elevated lactate, and risk factors for ischaemia.
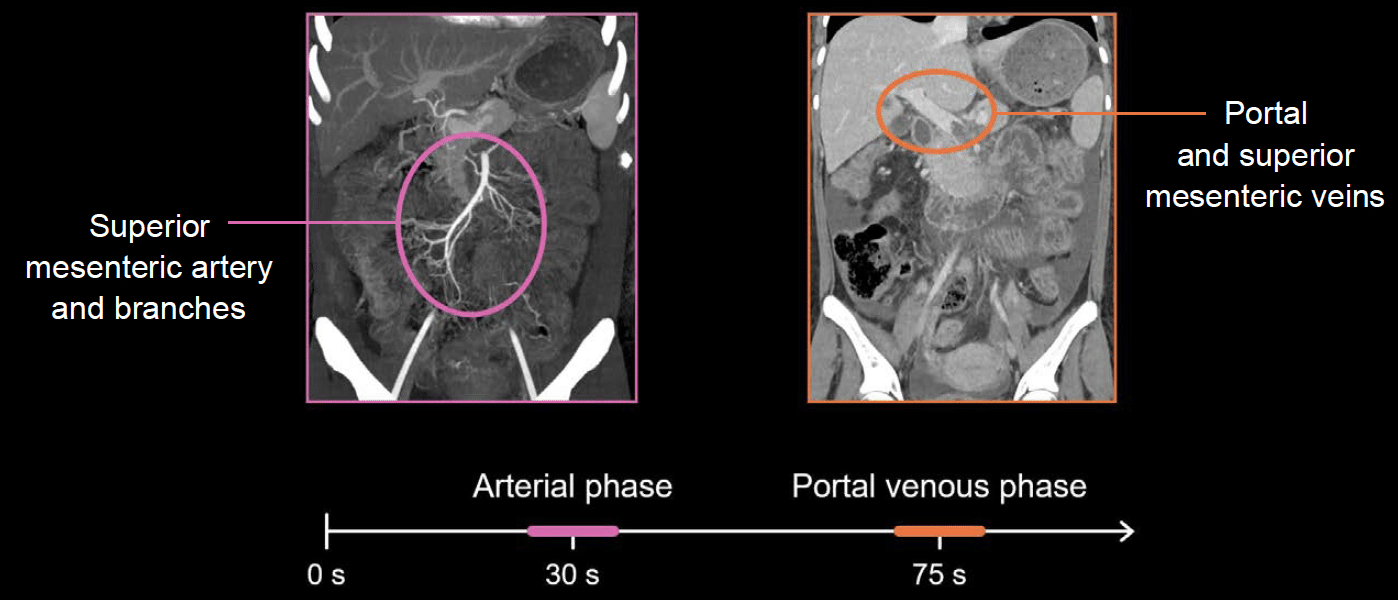
Most protocols for mesenteric ischaemia include images in the late arterial and portal venous phases. This examination is intended to focus on the superior mesenteric artery and its distal branches as well as the portal and superior mesenteric veins to make sure they are open, as patients could have arterial or venous ischaemia.
We also need to carefully evaluate the intestine for signs of abnormal thickening or enhancement, which can indicate ischaemia. Both increased and decreased enhancement can be seen with ischaemia, and looking at both late arterial and portal venous phase enhancement is helpful.
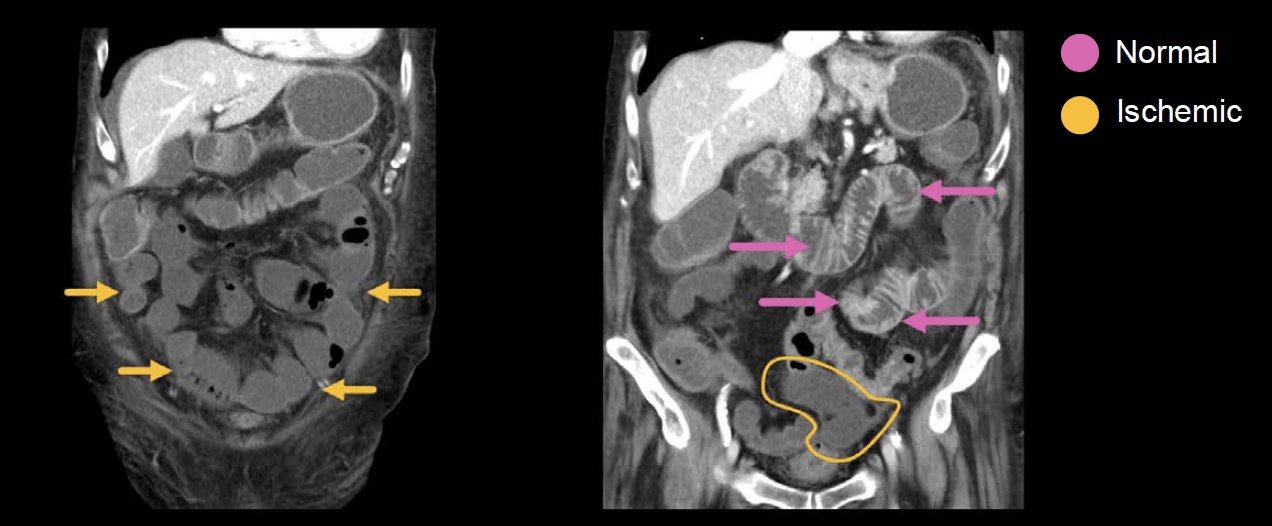
In the example below, the patient has acute blockage of the superior mesenteric artery. As a result, most of the small bowel has become ischaemic and so the bowel is not enhancing, and it blends in with the fluid inside of the bowel loops.
It can be particularly helpful to compare areas of suspected ischaemia to normal enhancing bowel walls, which are much brighter than the ischaemic loops, to confirm that these darker loops are abnormal.
The portal venous phase also provides complete anatomic imaging to check for any other cause of abdominal pain, as there is often something other than ischaemia to blame for the patient’s presentation (e.g. peptic ulcer disease, appendicitis, or diverticulitis).
Example 2: gastrointestinal bleeding
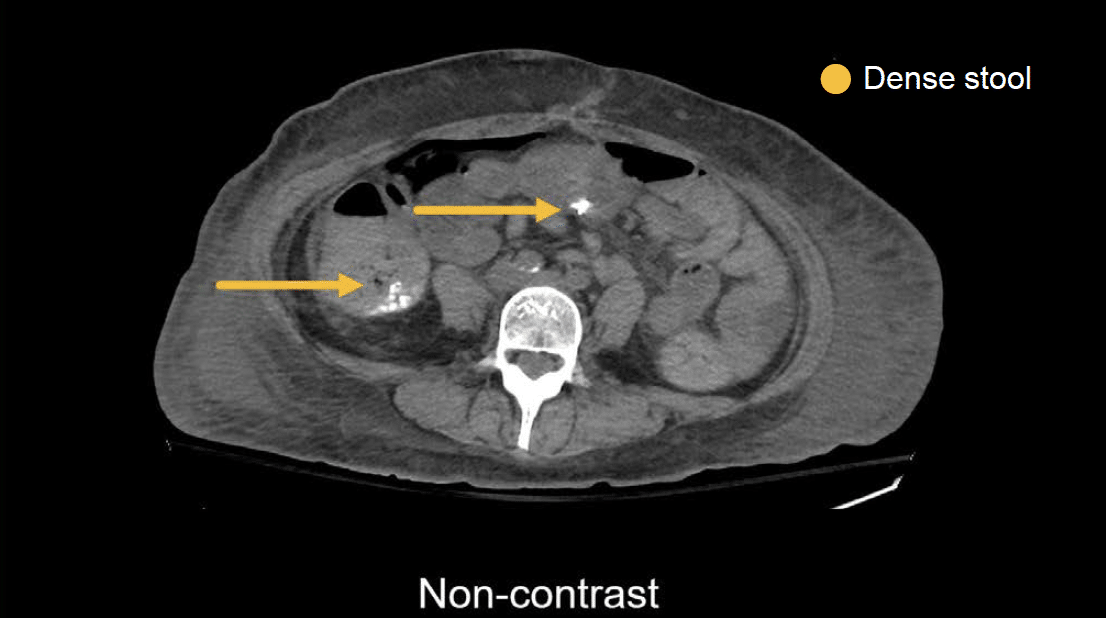
Multiphasic exams are also commonly used in patients with gastrointestinal bleeding, to look for the cause of bleeding. It is similar to the mesenteric ischaemia protocol with one addition – a non-contrast series. The non-contrast sequence allows you to dismiss any dense stool in the gastrointestinal tract that might mimic bleeding.
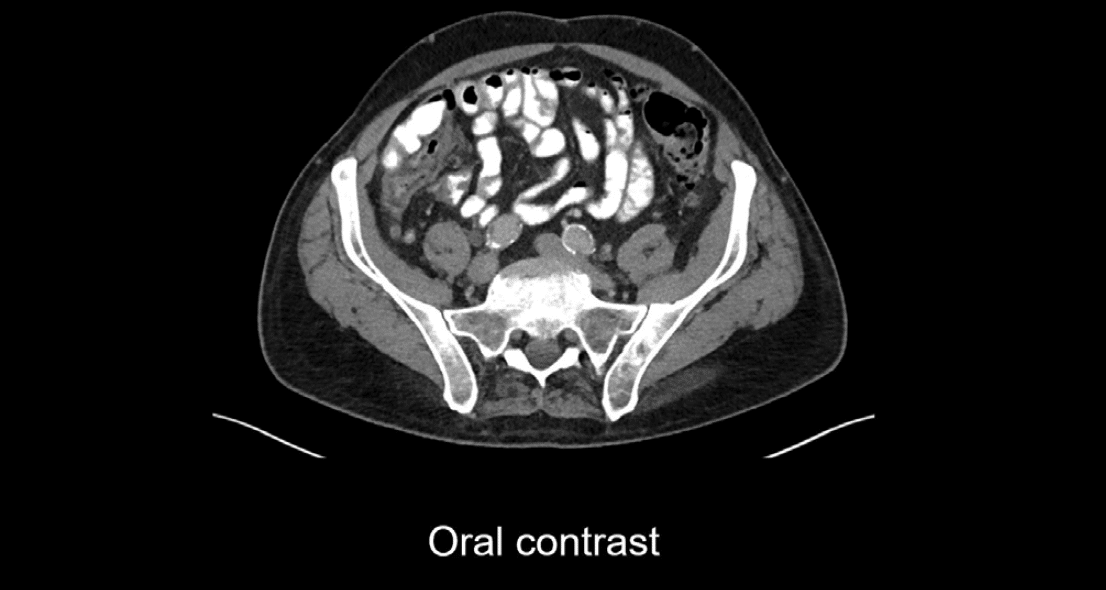
You may have guessed that we do not want to give oral contrast for these exams. As you can see below, the bright oral contrast in the small bowel would definitely hide any potential sites of bleeding, as both the contrast and any blood will appear bright.
Evaluating the vasculature at two time points allows you to see the contrast entering the bowel and spreading out over time. This is how you can confidently diagnose a site of bleeding.
In the example below, bright contrast enters the large intestine during the arterial phase and spreads out during the portal venous phase. Notice there is no dense material on the non-contrast series. Thus, we can confidently diagnose active bleeding in the large intestine with these three phases.
Example 3: acute aortic pathology
The final multiphasic exam in the emergency setting is to evaluate for acute aortic pathology such as a dissection or an abdominal aortic aneurysm (AAA), which is an abnormally dilated aorta with the potential to rupture.
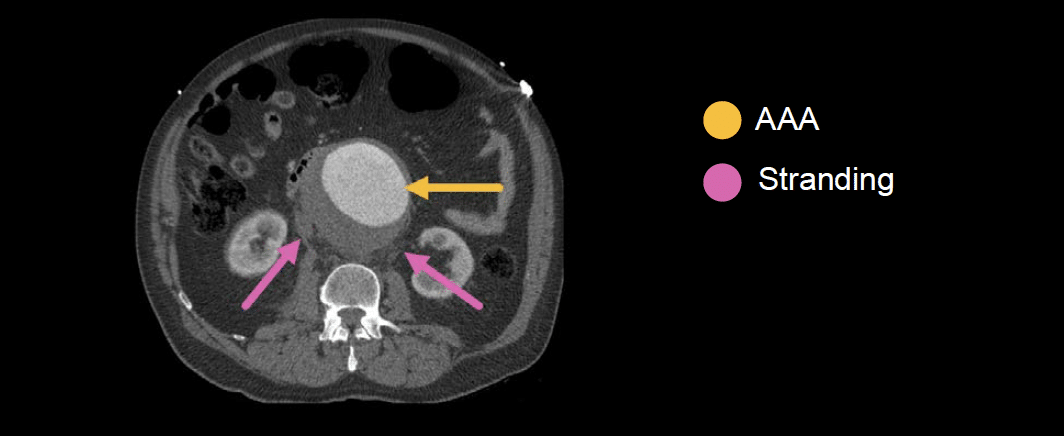
The image below shows a large aneurysm, and the stranding around it indicates that it has ruptured. This patient requires urgent surgery.
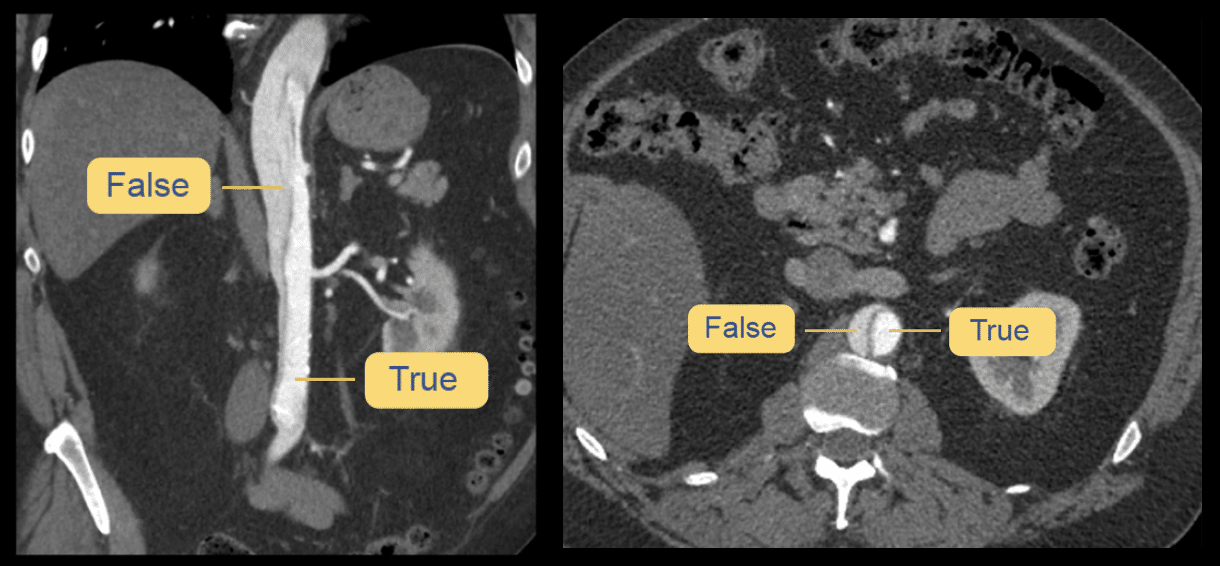
A dissection occurs when there is a tear in the inner layer of the aortic wall. This leads to the formation of a true lumen and a false lumen in the aortic wall. On CT, you will see a line (i.e. the intimal flap) separating the two. The false lumen is often larger and will appear darker than the true lumen because of decreased blood flow and contrast mixing.
While a rupturing or dissecting abdominal aorta can be diagnosed on a single portal venous phase (or even a non-contrast) exam, a complete vascular evaluation will usually include non-contrast, arterial, and portal venous phases. This is similar to the gastrointestinal bleeding study.
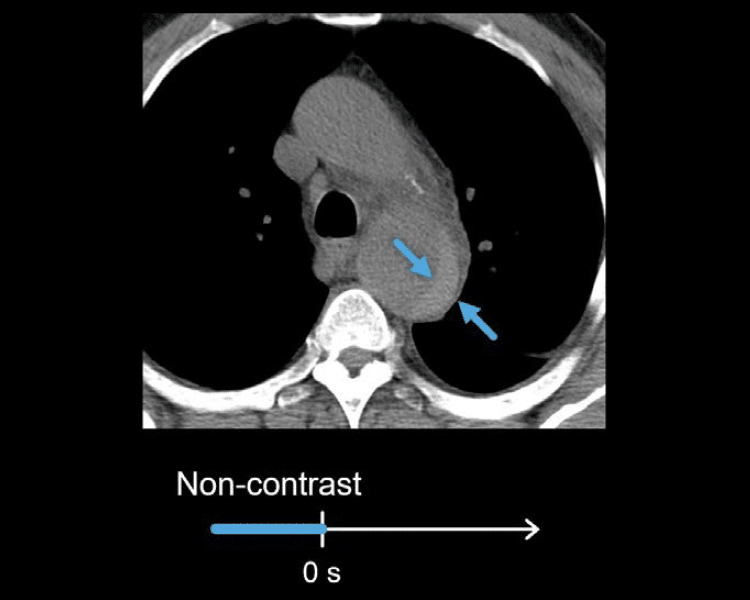
Non-contrast phase
The non-contrast image can help identify bleeding between the inner and outer walls of the aorta (i.e. an intramural haematoma). This aortic injury will appear crescent-shaped with increased density.
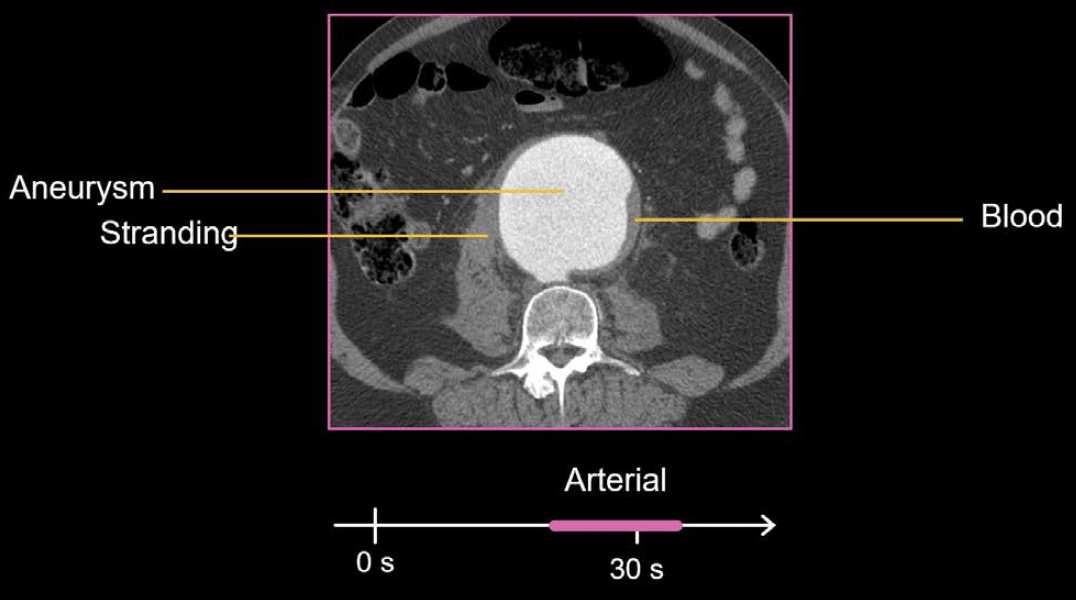
Arterial phase
The arterial phase provides the best evaluation of vascular openness (i.e. patency) and can show blood leakage and other early signs of a rupture. In the example shown next, the patient has a very large aneurysm with stranding and blood surrounding the aorta, indicating rupture.
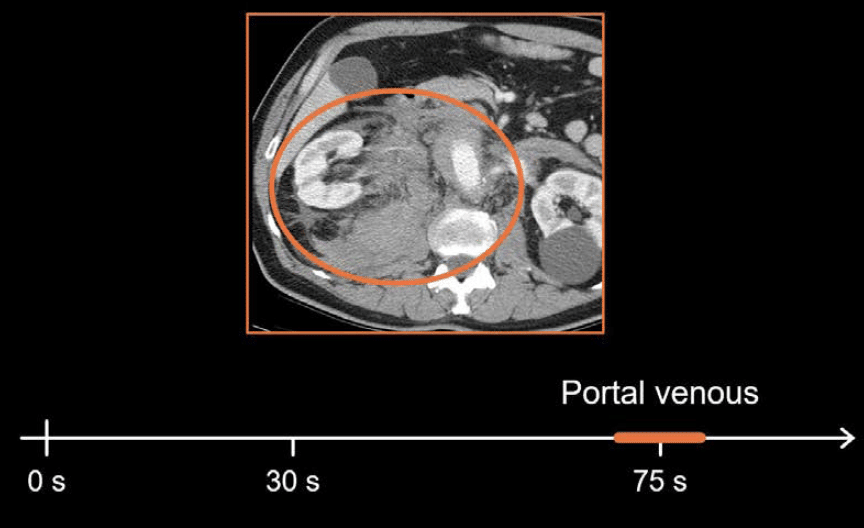
Portal venous phase
The portal venous phase helps complete the evaluation by showing solid organ and bowel enhancement. Acute aortic pathology can lead to ischaemia or infarct of the organs and bowel, which is best detected during the portal venous phase. It also helps you to look for other causes of acute abdominal pain if the vascular evaluation is normal.
Although these CT exams are used in different clinical scenarios, they are quite similar. They all include the arterial and portal venous phases. When looking for bleeding, as in gastrointestinal bleeding and acute aortic pathologies, a non-contrast sequence is also typically captured.
This is an edited excerpt from the Medmastery course Abdominal CT Essentials by Michael P. Hartung, MD. Acknowledgement and attribution to Medmastery for providing course transcripts.
- Hartung MP. Abdominal CT: Common Pathologies. Medmastery
- Hartung MP. Abdominal CT: Essentials. Medmastery
- Hartung MP. Abdomen CT: Trauma. Medmastery
References
- Top 100 CT scan quiz. LITFL
Radiology Library: Abdominal CT Basics
- Hartung MP. Abdominal CT: Phases. LITFL
- Hartung MP. Abdominal CT: Cancer staging. LITFL
- Hartung MP. Abdominal CT: GU imaging. LITFL
- Hartung MP. Abdominal CT: Urogram. LITFL
- Hartung MP. Abdominal CT: Cystogram. LITFL
- Hartung MP. Abdominal CT: Flank pain imaging. LITFL
Abdominal CT interpretation

Assistant Professor of Abdominal Imaging and Intervention at the University of Wisconsin Madison School of Medicine and Public Health. Interests include resident and medical student education, incorporating the latest technology for teaching radiology. I am also active as a volunteer teleradiologist for hospitals in Peru and Kenya. | Medmastery | Radiopaedia | Website | Twitter | LinkedIn | Scopus

MBChB (hons), BMedSci - University of Edinburgh. Living the good life in emergency medicine down under. Interested in medical imaging and physiology. Love hiking, cycling and the great outdoors.

Muy bueno el Documento. Gracias