
![]()
Abdominal CT: necrotizing pancreatitis
Recognizing acute necrotizing pancreatitis
The degree of enhancement of the pancreas will enable you to differentiate between interstitial and necrotizing pancreatitis. It is important to recognize necrotizing pancreatitis as it is associated with a greater risk of complications and requires more aggressive management and close follow-up.
Key findings for acute necrotizing pancreatitis
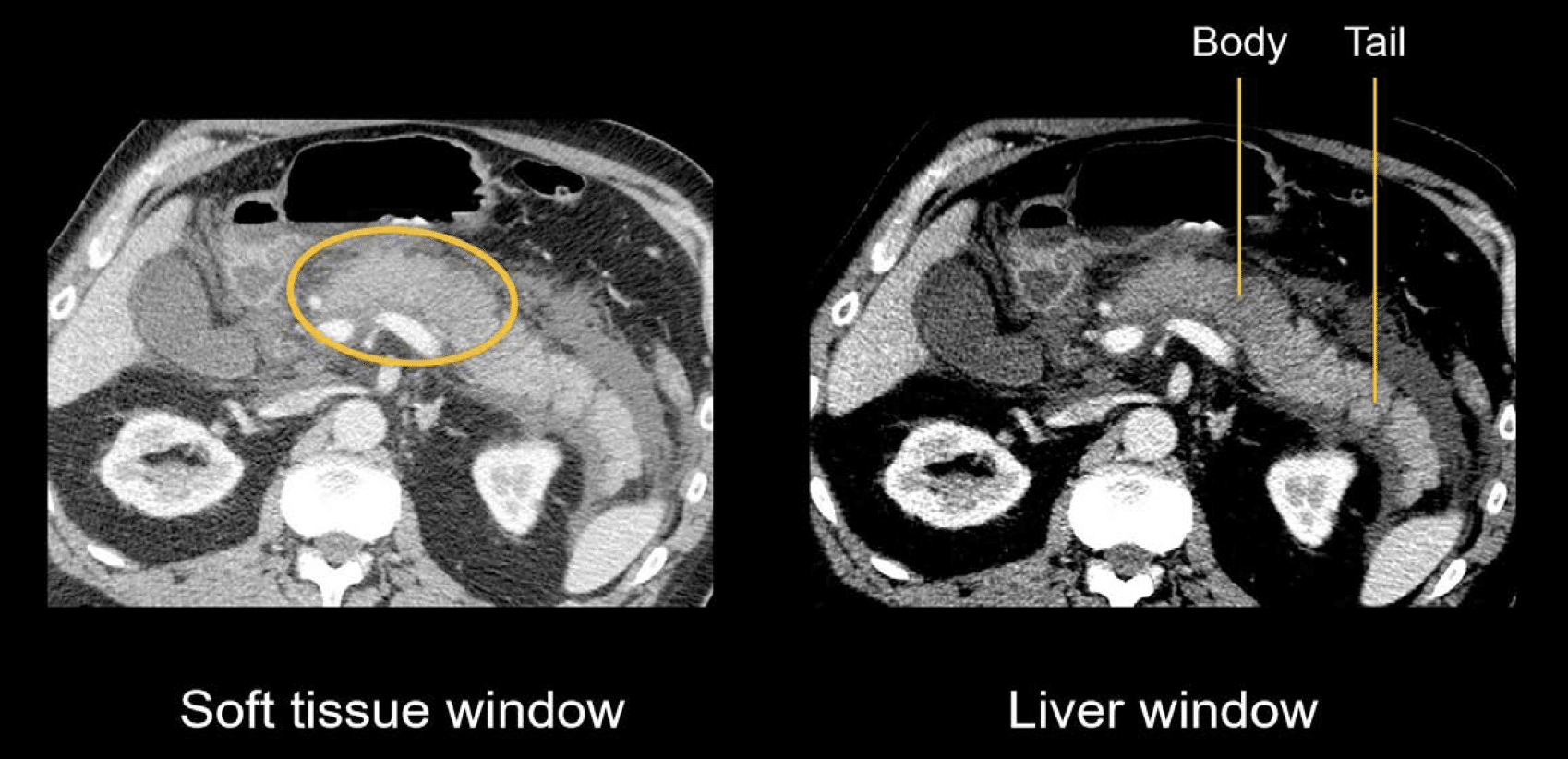
Decreased or absent enhancement of the pancreas on CT defines necrosis. Take a look at the case below. By using the liver window settings, the differences in soft tissue contrast are made more apparent, making it easier to identify necrosis. The liver window helps us to see the transition from decreased enhancement in the pancreas body to the normally enhancing pancreas tail.
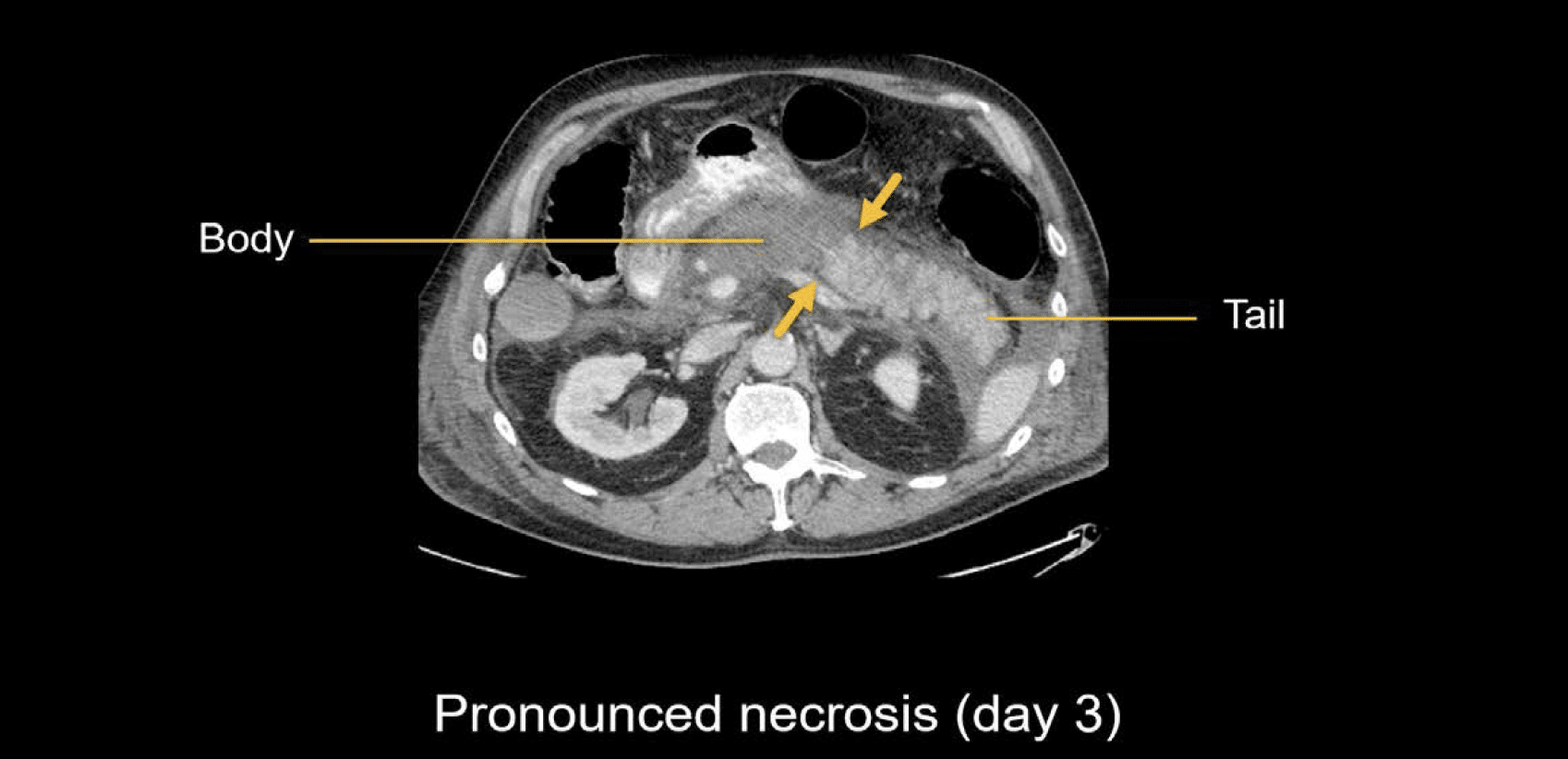
If you are unsure, it is perfectly reasonable to recommend a short interval followup scan. Over time, those subtle differences will become more apparent. In this same case, the necrosis became much more apparent by day three, with a clear delineation between the non-enhancing pancreas body and the enhancing tail.
Clinical Case 1
Scroll through these images from a patient presenting with severe abdominal pain. Focus on evaluating pancreas enhancement and see if we can determine if there is necrosis or not.
- Start by choosing to look at the axial and coronal images side-by-side to help your understanding of the anatomy.
- As you start scrolling down the abdomen on the axial view, you will see that there is fluid surrounding the liver and spleen.
- Scrolling around the pancreas, you’ll notice there is quite a lot of fluid and stranding surrounding it in the retroperitoneum and in the mesentery.
- Carefully review the pancreas tissue. Notice that there is decreased or absent enhancement of much of the pancreas head, neck, and body.
- See how the uncinate process and distal body and tail are enhancing.
- Take a look at those same findings on the coronal view.
- These findings are diagnostic for necrotizing pancreatitis involving a rather large portion of the pancreas.
Key findings for the late stage of acute pancreatitis
When acute pancreatitis first develops, the fluid, stranding, and inflammation are not particularly organized. However, the body will respond over time by forming a wall around these collections, effectively organizing them.
Over a period of about four weeks (or longer), both interstitial and necrotizing pancreatitis can progress to later forms with well-defined organized collections.
Pseudocysts
In the case of interstitial pancreatitis, the collections are called pseudocysts and are comprised of organized fluid from pancreatic enzymes. These are separate from the pancreas but can surround, displace, and compress other structures.
The very large pseudocyst shown below is in front of the pancreas and is significantly compressing the stomach.

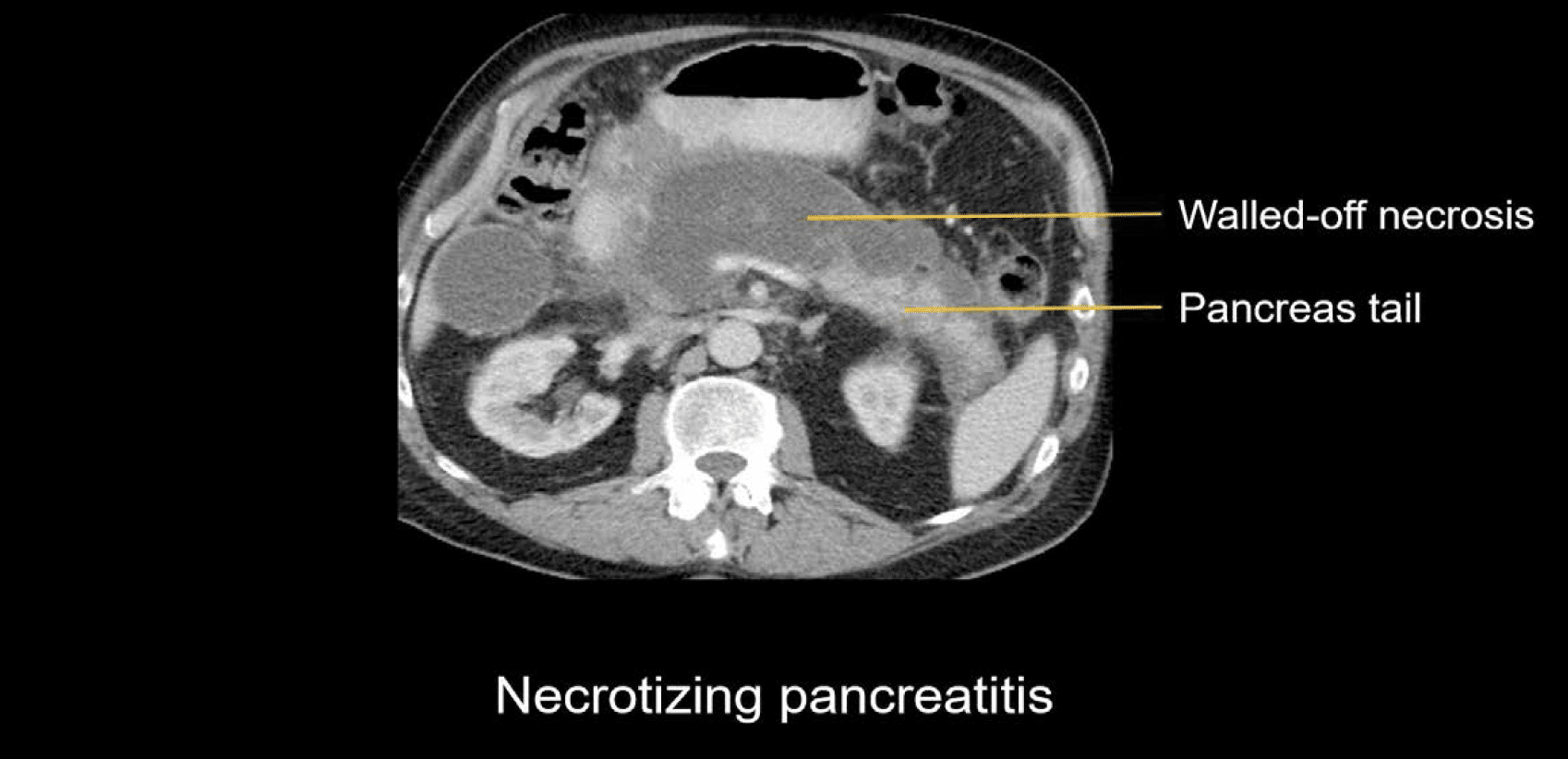
Walled-off necrosis
In the case of necrotizing pancreatitis, the collections are called walled-off necrosis and are comprised of necrotic debris from the pancreas or surrounding fat. These collections usually take the place of the necrotic pancreas tissue, but you will often see small segments of remaining enhancing pancreas nearby, such as the tail in the example shown next.
Both types of collections can become infected and drainage may be considered. Drainage can be performed through the skin or directly into the stomach with a special stent.
This is an edited excerpt from the Medmastery course Abdominal CT Pathologies by Michael P. Hartung, MD. Acknowledgement and attribution to Medmastery for providing course transcripts
- Hartung MP. Abdominal CT: Common Pathologies. Medmastery
- Hartung MP. Abdominal CT: Essentials. Medmastery
- Hartung MP. Abdomen CT: Trauma. Medmastery
References
- Top 100 CT scan quiz. LITFL
Radiology Library: Acute abdomen. Solid organ and Vascular pathology
- Hartung MP. Abdominal CT: acute interstitial pancreatitis
- Hartung MP. Abdominal CT: acute necrotizing pancreatitis
- Hartung MP. Abdominal CT: renal stones and the flank pain CT
- Hartung MP. Abdominal CT: renal infections
- Hartung MP. Abdominal CT: cholecystitis
- Hartung MP. Abdominal CT: intestinal ischaemia
- Hartung MP. Abdominal CT: rupturing abdominal aortic aneurysm
Abdominal CT interpretation

Assistant Professor of Abdominal Imaging and Intervention at the University of Wisconsin Madison School of Medicine and Public Health. Interests include resident and medical student education, incorporating the latest technology for teaching radiology. I am also active as a volunteer teleradiologist for hospitals in Peru and Kenya. | Medmastery | Radiopaedia | Website | Twitter | LinkedIn | Scopus

MBChB (hons), BMedSci - University of Edinburgh. Living the good life in emergency medicine down under. Interested in medical imaging and physiology. Love hiking, cycling and the great outdoors.