
![]()
Abdominal CT: renal infections
Spotting renal infections
Pyelonephritis is caused by an infection of the urinary tract that starts in the bladder and works its way up to the kidneys through the ureters. Less commonly, it can also be caused by an infection carried in the blood.
While CT is not necessary to make this diagnosis, it can be helpful for ruling out complicated forms of pyelonephritis which may require invasive procedures (such as abscess drainage) or surgical intervention (such as removal of the infected kidney in rare, very severe cases).
Key findings
There are three key imaging findings to look for when diagnosing pyelonephritis
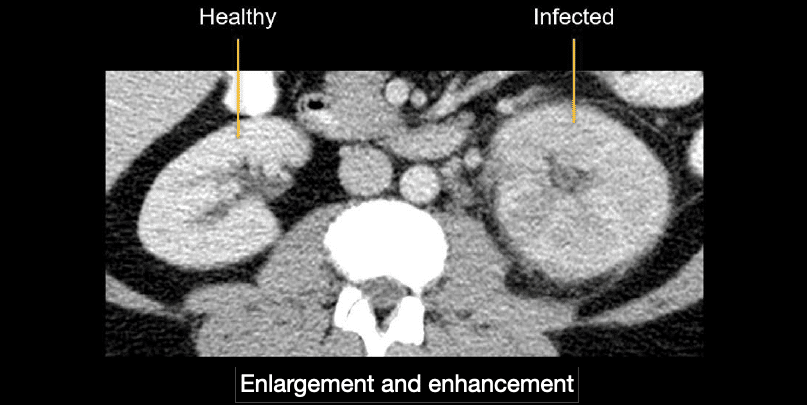
- Enlargement and abnormal enhancement of the infected kidney
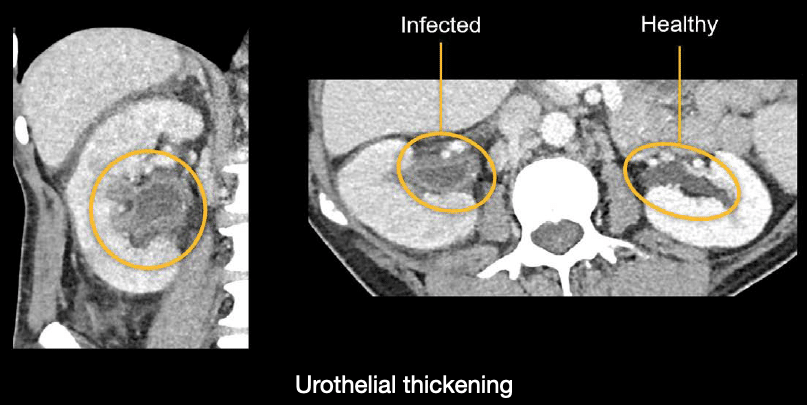
- Thickening and inflammation of the urothelium or ureter
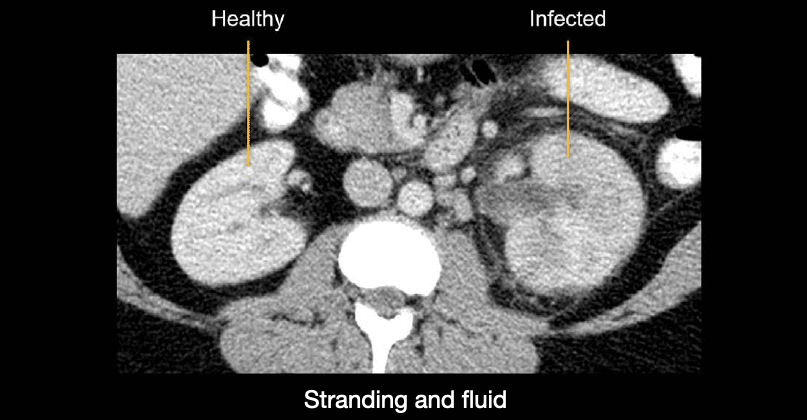
- Reactive stranding and fluid surrounding the infected kidney
Enlargement and abnormal enhancement of the infected kidney. This is best appreciated by comparing the kidneys side by side. The infected kidney will look swollen and enhance less than the normal, healthy kidney.
Thickening and inflammation of the urothelium or ureter. The urothelium is the inner lining of the urinary tract. In the case of inflammation of either the urothelium or ureter, there is thickening and increased enhancement of the renal pelvis. In the example shown next, you can compare the affected right side to the normal left side.
Reactive stranding and fluid surrounding the infected kidney Notice below how the affected left side compares to the clean fat that surrounds the normal right kidney.
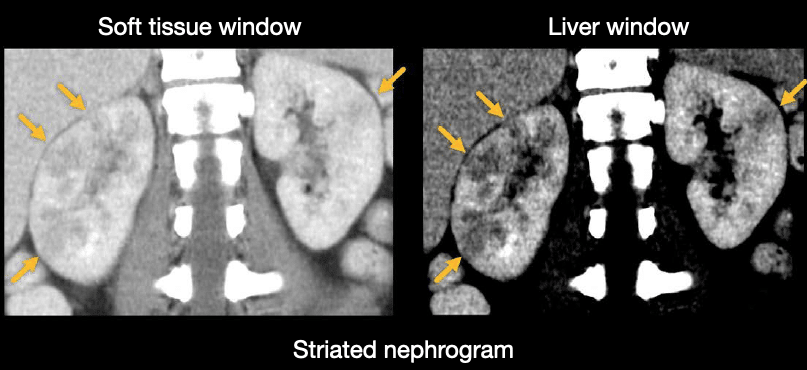
Infection will cause the kidney to enhance less, often in patches or lines radiating from the renal hilum and into the cortex. This pattern of enhancement is referred to as a striated nephrogram. It can be relatively subtle but is easiest to see when using liver windows and viewing both kidneys on coronal images.
Knowledge iteration
Case 1
Scroll through these PACS viewer images
- Start by choosing to view axial and coronal images side-by-side.
- Notice that while both kidneys are involved, the right is worse than the left.
- There is also mild stranding in the fat surrounding the right kidney.
- The cortex has abnormal areas of decreased enhancement corresponding to areas of infection, but these are relatively subtle.
- By focusing on the coronal images and using a narrow liver window to accentuate differences in soft tissue contrast, you can more confidently evaluate the areas of infection.
- The diagnosis in this case is bilateral uncomplicated pyelonephritis
Complicated pyelonephritis
Now that we have discussed uncomplicated pyelonephritis, let’s talk about the major complications we need to look for. These can drive urgent intervention rather than relying on antibiotic therapy alone.
Abscess
One complication you will need to watch for is an abscess. In the example below, the abscess looks like a lobulated, enhancing fluid collection arising from the renal cortex.

Renal abscesses commonly start as smaller microabscesses that can come together (i.e., coalesce) to form large collections over time. Unlike larger abscesses, most of these smaller abscesses are not drainable, but they can be monitored after antibiotic therapy to ensure resolution.

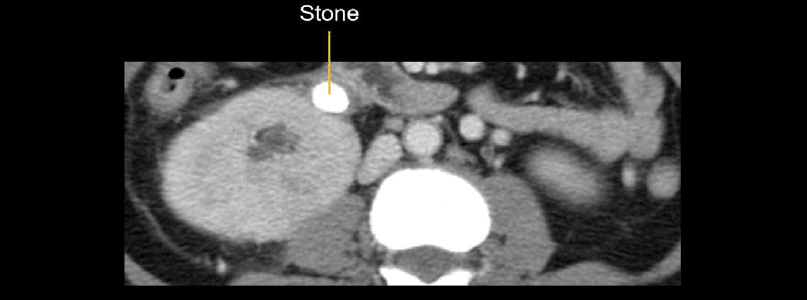
Obstruction
You will also want to be on the lookout for a stone causing an obstruction. This is a surgical emergency requiring decompression of the obstructed and infected kidney.
Note: While it is helpful to diagnose pyelonephritis by comparing the kidneys side-by-side, there are cases where both kidneys can be involved, so be careful!
Less common forms of pyelonephritis
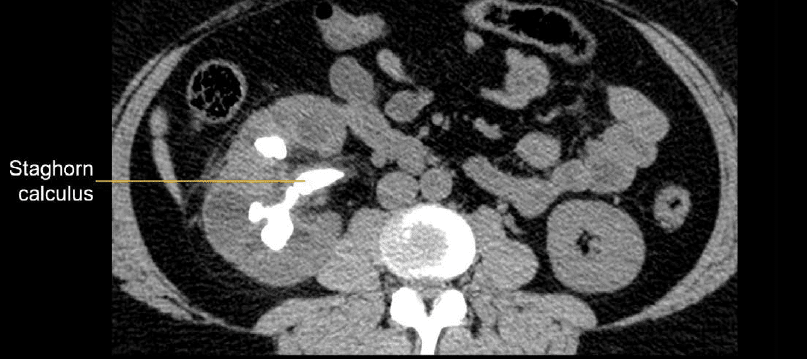
Xanthogranulomatous pyelonephritis
This is caused by chronic obstruction and infection of the kidney—often due to a central stone called a staghorn calculus that can branch.
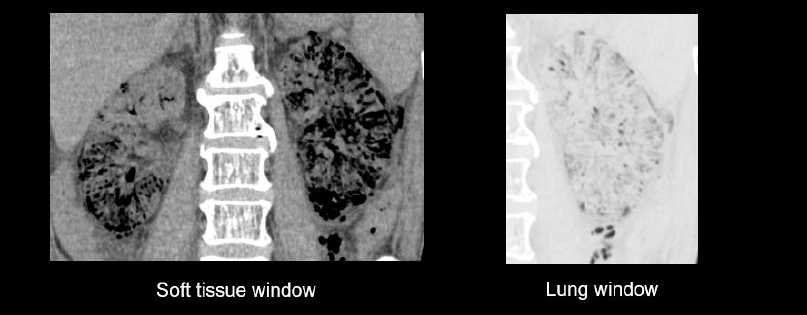
Emphysematous pyelonephritis
This is a very severe infection where gas forms in the kidney. The major risk factor for developing this is type 2 diabetes. Notice in the image below how dark the gas looks with the soft tissue versus the lung window settings
Both are rare forms of pyelonephritis which often require surgical resection of the infected kidney
Knowledge iteration
Let’s review a close look at an example of complicated pyelonephritis with this online PACS viewer link
- Start by choosing to view the axial and coronal images side-by-side.
- Scroll down to the kidneys and notice that the left kidney is a good deal larger than the right.
- Notice also that the left kidney has many striations and cortical fluid collections representing coalescing microabsesses, and there is stranding in the surrounding fat.
- Don’t forget the right kidney! Did you notice the subtle areas of decreased enhancement?
- Switching to the liver window will help you to see these areas better.
- This case provides an excellent comparison of uncomplicated right and complicated left pyelonephritis.
This is an edited excerpt from the Medmastery course Abdominal CT Pathologies by Michael P. Hartung, MD. Acknowledgement and attribution to Medmastery for providing course transcripts
- Hartung MP. Abdominal CT: Common Pathologies. Medmastery
- Hartung MP. Abdominal CT: Essentials. Medmastery
- Hartung MP. Abdomen CT: Trauma. Medmastery
References
- Top 100 CT scan quiz. LITFL
- Xanthogranulomatous Pyelonephritis. LITFL
Radiology Library: Acute abdomen. Solid organ and Vascular pathology
- Hartung MP. Abdominal CT: acute interstitial pancreatitis
- Hartung MP. Abdominal CT: acute necrotizing pancreatitis
- Hartung MP. Abdominal CT: renal stones and the flank pain CT
- Hartung MP. Abdominal CT: renal infections
- Hartung MP. Abdominal CT: cholecystitis
- Hartung MP. Abdominal CT: intestinal ischaemia
- Hartung MP. Abdominal CT: rupturing abdominal aortic aneurysm
Abdominal CT interpretation

Assistant Professor of Abdominal Imaging and Intervention at the University of Wisconsin Madison School of Medicine and Public Health. Interests include resident and medical student education, incorporating the latest technology for teaching radiology. I am also active as a volunteer teleradiologist for hospitals in Peru and Kenya. | Medmastery | Radiopaedia | Website | Twitter | LinkedIn | Scopus

MBChB (hons), BMedSci - University of Edinburgh. Living the good life in emergency medicine down under. Interested in medical imaging and physiology. Love hiking, cycling and the great outdoors.