
![]()
Activate or Wait – 005
45 year-old man with two hours of central crushing chest pain. Smoker, significant family history of ischaemic heart disease.
ETA 20 minutes.

Would you activate your cath lab/STEMI protocol?
0
ECG interpretation
Anteroseptal OMI
- ST elevation in leads V1-V3
- Reciprocal ST depression in inferior leads, most notable in lead III
- Hyperacute T-waves in V2-V5 with a very low preceding QRS amplitude. These two components make for a very large T/R ratio
- Reverse R wave progression (smaller in V3 than V2)
- “Down-up” T wave in lead III and aVF
These ECG changes may be easily mistaken for benign early repolarisation (BER) given the patient age and asymmetrical nature of T waves. However, as discussed in case 001, we should not diagnose BER when there is ST depression in leads other than aVR.
If there is ongoing doubt about whether anterior ST elevation represents LAD occlusion or BER, we can use the validated 4-variable subtle anterior OMI formula to differentiate between the two (see clinical pearls below). In this case, a score of 20.1 strongly suggests
AI interpretation by PMcardio
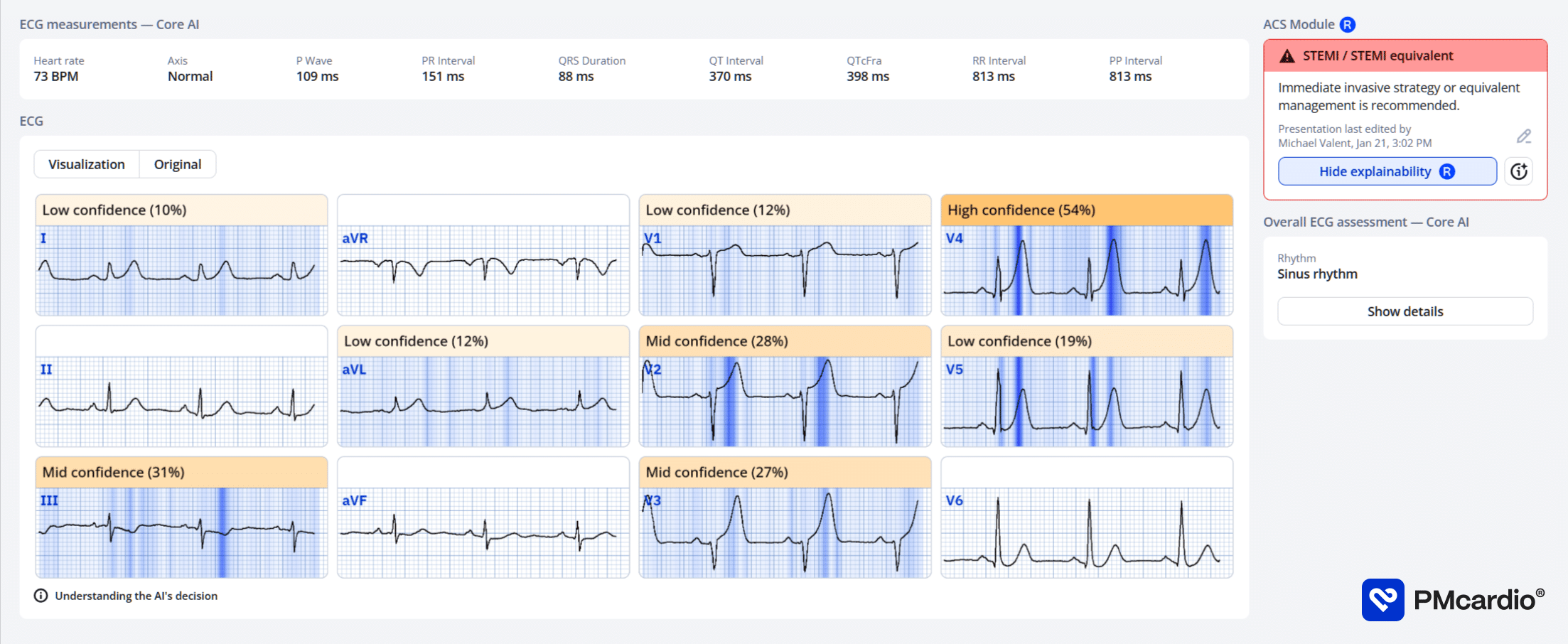
PMcardio’s AI ECG model identified a STEMI/STEMI equivalent.
The explainability feature offers insights into problematic patterns in the respective leads, providing a clear rationale for the diagnosis.
Further reading
Outcome
Key Finding:
Occluded mid left anterior descending (LAD) artery
Findings:
- Left Main Coronary Artery – short. Widely patent.
- Left Anterior Descending Coronary Artery – type III vessel. 50% proximal stenosis. Occluded from mid-vessel. Thrombotic. Culprit.
- Left Circumflex Coronary Artery – large calibre vessel. Mild disease.
- Right Coronary Artery – medium calibre vessel. Dominant. Moderate mid vessel disease.
- Left Ventriculogram – systolic function 45% anterolateral hypokinesis.
Plan:
- Occluded LAD (culprit). Proceeded to PCI of mid LAD
Clinical Pearls
Early presentations of acute occlusion myocardial infarction may not always meet traditional STEMI criteria. Examine closely for reciprocal ST depression and hyperacute T waves which may be the most prominent initial findings.
The 4-variable subtle anterior STEMI formula is a validated tool that can be used to assist in differentiating “normal variant” ST elevation from LAD occlusion. Scores above 18 are strongly suggestive of anterior STEMI.
Points are added for:
- Corrected QT interval
- ST elevation in V3 60mm after the J point
Points are subtracted for:
- QRS amplitude in V2
- R amplitude in V4
In LAD occlusion:
- QTc will be more prolonged due to ischaemia
- Convex/horizontal nature of ST elevation will produce more pronounced ST elevation in V3 than the concave nature of normal variant ST elevation
- Poor R wave progression will result in smaller R wave amplitude in V4, and smaller QRS complexes
- Consider using the formula in patients with a concerning presentation for ACS that have prominent anterior ST elevation but absence of inferior reciprocal change.
Read more about the original study here, and external validation of the formula here.
References
Further reading
- Driver BE, Khalil A, Henry T, Kazmi F, Adil A, Smith SW. A new 4-variable formula to differentiate normal variant ST segment elevation in V2-V4 (early repolarization) from subtle left anterior descending coronary occlusion – Adding QRS amplitude of V2 improves the model. J Electrocardiol. 2017 Sep-Oct;50(5):561-569.
- Bozbeyoğlu E, Aslanger E, Yıldırımtürk Ö, Şimşek B, Karabay CY, Şimşek MA, Tekkeşin Aİ, Değertekin M, Kozan Ö. A tale of two formulas: Differentiation of subtle anterior MI from benign ST segment elevation. Ann Noninvasive Electrocardiol. 2018 Nov;23(6):e12568.
- Burns E, Buttner R. Anterior Myocardial Infarction. LITFL
- Burns E, Buttner R. T wave. LITFL
- Nickson C. STEMI Management. LITFL
Online resources
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Smith SW. Dr Smith’s ECG blog.
- Rawshani A. Clinical ECG Interpretation ECG Waves
ACTIVATE or WAIT
EKG Interpretation

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.

Dr. Stephen W. Smith is a faculty physician in the Emergency Medicine Residency at Hennepin County Medical Center (HCMC) in Minneapolis, MN, and Professor of Emergency Medicine at the University of Minnesota. Author of Dr Smith's ECG Blog | Bibliography | X |

Dr. Robert Herman is the Co-founder and Chief Medical Officer of PMcardio by Powerful Medical. He is a cardiovascular researcher at the Cardiovascular Center Aalst in Belgium, specializing in applying AI to enhance the detection and referral of cardiovascular patients. LinkedIn | X (formerly Twitter) | Get in Touch