
![]()
Benign Early Repolarisation
Benign early repolarisation (BER) is a usually benign ECG pattern producing widespread ST segment elevation that is commonly seen in young, healthy patients < 50 years of age. Also known as “high take-off” or “J-point elevation”, it may mimic pericarditis or acute MI.
ECG Features
- Widespread concave ST elevation, most prominent in the mid-to-left precordial leads (V2-5)
- Notching or slurring at the J point
- Prominent, slightly asymmetrical T waves that are concordant with the QRS complex
- ST elevation : T wave height ratio in V6 < 0.25 (see below)
- No reciprocal ST depression to suggest Occlusion MI
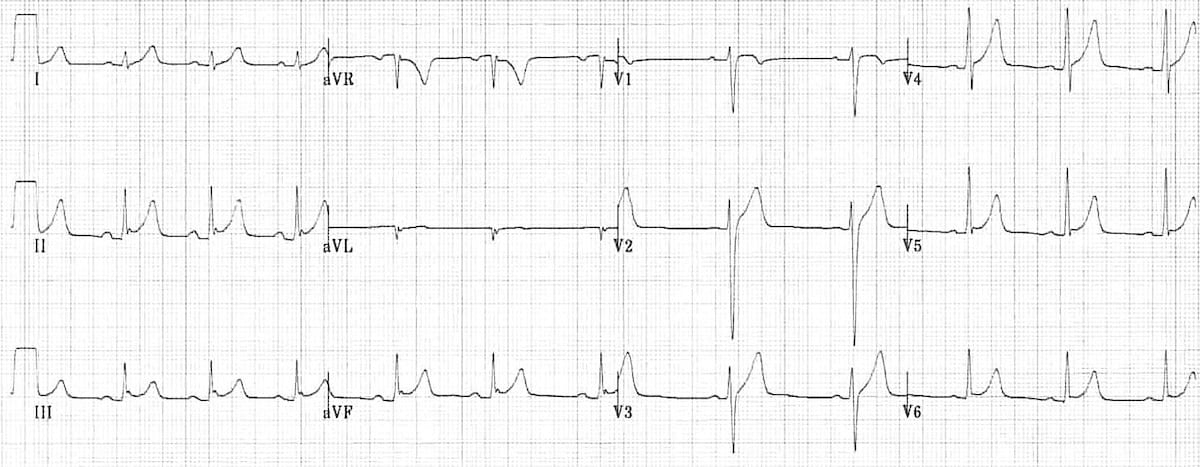
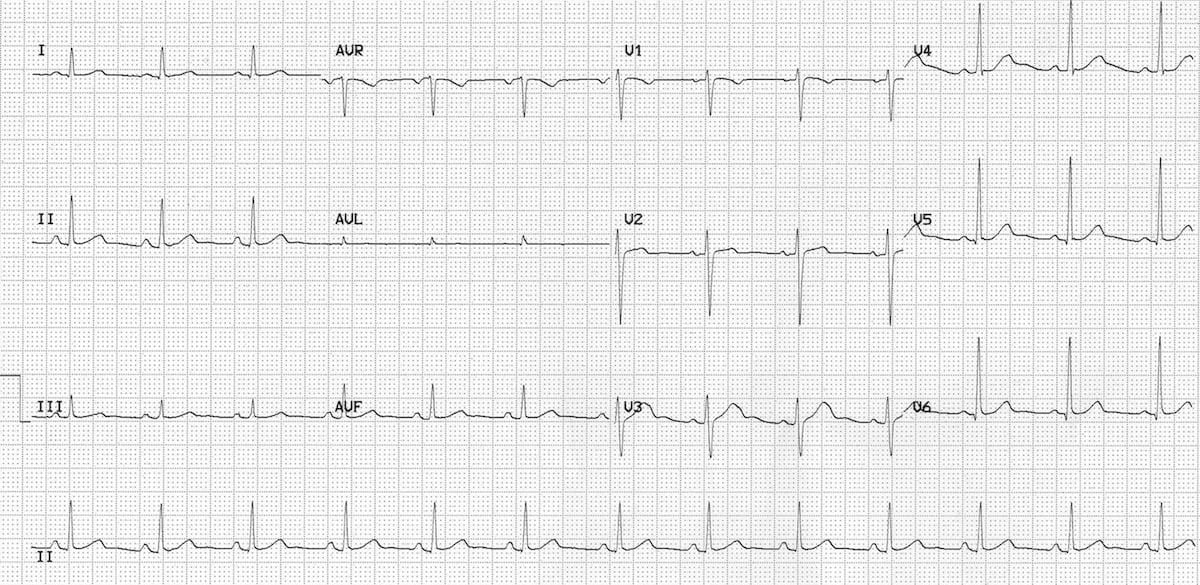
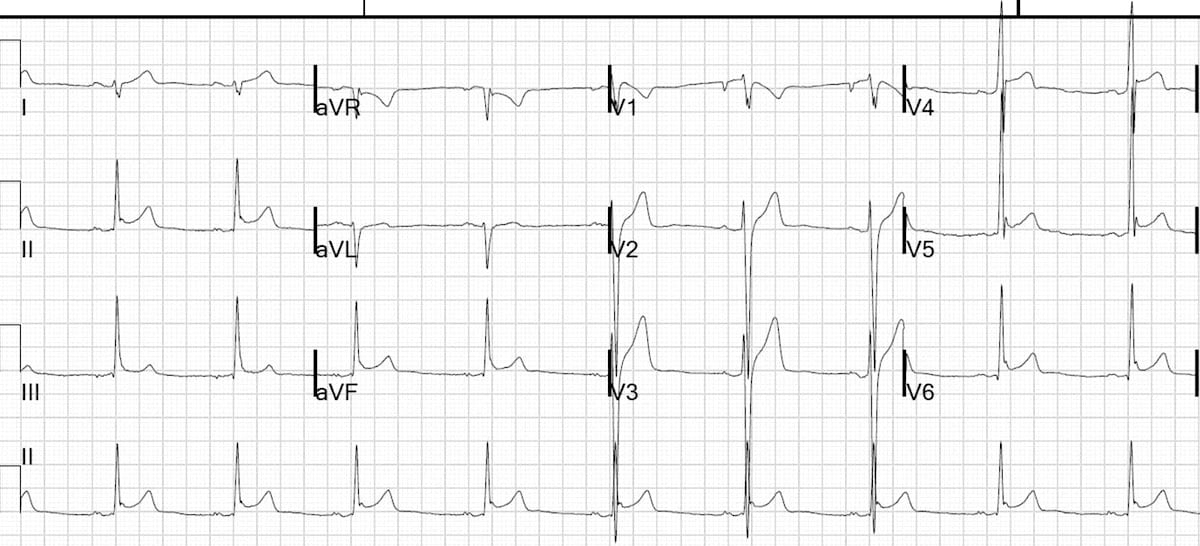
1) Generalised concave ST elevation in precordial (V2-6) and limb leads (I, II, III, aVF)
2) J-point notching is evident in the inferior leads (II, III and aVF)
3) ST elevation : T wave ratio < 0.25 in V6
Clinical Relevance
- Widespread ST elevation in BER may mimic pericarditis or acute MI
- Up to 10-15% of ED patients presenting with chest pain will have BER on their ECG, making it a common diagnostic challenge for clinicians. BER is less common in patients over 50, and particularly rare in those over 70, wherein ST elevation is more likely to represent myocardial ischaemia
- The physiological basis of BER is poorly understood. It is generally thought to be a normal variant that is not indicative of underlying cardiac disease, but recently a link has been made between the global BER pattern and future risk of idiopathic ventricular fibrillation (VF)
Avoid diagnosing BER in patients over the age of 50, especially those with risk factors for ischaemic heart disease.
ST segment / T wave morphology
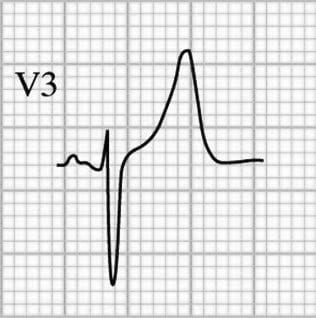
The ST segment-T wave complex in BER has a characteristic appearance:
- There is elevation of the J point
- The T wave is peaked and slightly asymmetrical
- The ST segment and the ascending limb of the T wave form an upward concavity
- The descending limb of the T wave is straighter and slightly steeper than the ascending limb
The concept of “smiley-shaped” ST elevation, popularized by Ken Grauer in 1993, is worthy of mention:
“…smiley-shaped” ST elevation is a GREAT visual aid – but you may want to describe upward concavity or ST coving (downward convexity) to your consulting cardiologist (rather than “smiley” or “frowny”) so as to enhance your credibility. But “smiley” vs “frowny” ST segments works as a great descriptor among colleagues…
Typical morphology of BER

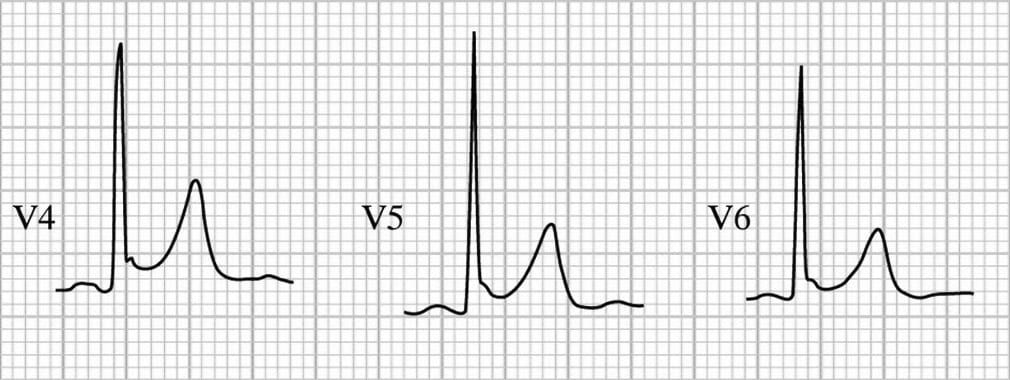
J-point morphology
One characteristic feature of BER is the presence of a notched or irregular J point: the so-called “fish hook” pattern. This is often best seen in lead V4.
Examples of J-point notching:

Temporal Stability of BER
Although the ST elevation of BER does not show rapid progression like STEMI, nor evolution over several weeks like pericarditis, the ECG pattern is not entirely static over time:
- The degree of ST elevation may fluctuate in response to changes in autonomic tone, diminishing with increased sympathetic tone / exercise / tachycardia or increasing when the heart rate slows
- The ST elevation may gradually disappear over time as the patient ages: up to 30% of patient with BER will have resolution of ST elevation on ECGs taken many years later
Variation with Heart Rate
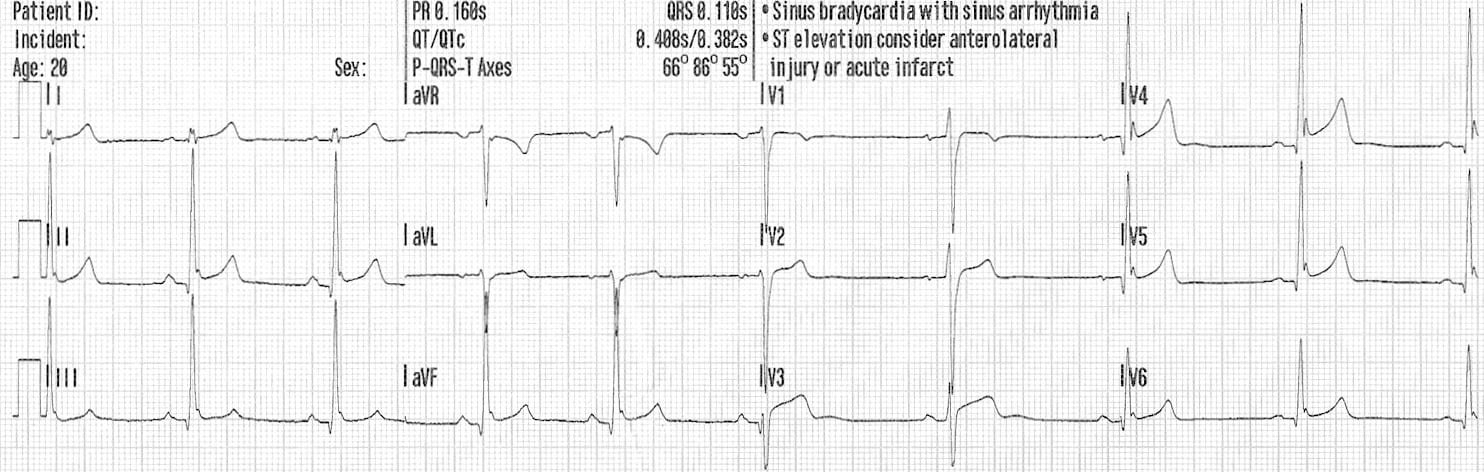
The following two ECGs were taken 24 hours apart from a healthy 17-year old female who was admitted to hospital following a benzodiazepine overdose. She had no chest pain, and cardiac biomarkers were normal. You can see how the ECG features of BER vary with the heart rate:
Example 1 (heart rate = 54 bpm)
- ST elevation and J-point notching are more prominent at a slower heart rate.
Example 2 (heart rate = 76 bpm)
- ST elevation and J-point notching become less prominent as the heart rate increases.
Check out this post on ST elevation of early depolarisation from Dr Smith’s ECG blog for another example of this interesting phenomenon.
Benign Early Repolarisation vs Pericarditis
Pericarditis can be difficult to differentiate from Benign Early Repolarisation (BER), as both conditions are associated with concave ST elevation. One useful trick to distinguish between these two entities is to look at the ST segment / T wave ratio and the Fish Hook Pattern.
ST segment / T wave ratio:
The vertical height of the ST segment elevation (from the end of the PR segment to the J point) is measured and compared to the amplitude of the T wave in V6:
- ST / T wave ratio of > 0.25 suggests pericarditis
- ST / T wave ratio of < 0.25 suggests BER
Example 1: Benign Early Repolarisation
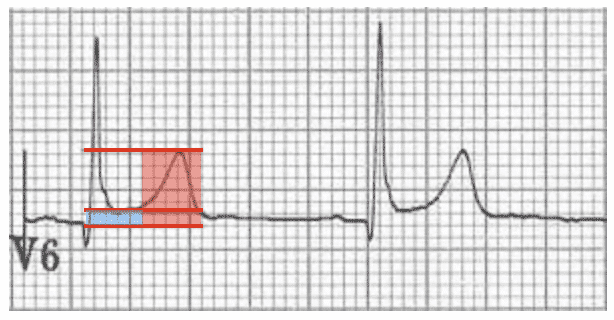
- ST segment height = 1 mm
- T wave height = 6 mm
- ST / T wave ratio = 0.16
- The ST / T wave ratio < 0.25 is consistent with BER
Example 2: Pericarditis

- ST segment height = 2 mm
- T wave height = 4 mm
- ST / T wave ratio = 0.5
- The ST / T wave ratio > 0.25 is consistent with pericarditis
Fish Hook Pattern
Another clue that suggests BER is the presence of a notched or irregular J point: the so-called “fish hook” pattern. This is often best seen in lead V4.
Differentiating between BER and pericarditis
| ECG Feature | Benign Early Repolarisation | Pericarditis |
| ST elevation | Limited to precordial leads | Generalised |
| PR depression | No | Yes |
| T wave amplitude | Prominent | Normal |
| ST segment / T wave ratio | < 0.25 | > 0.25 |
| “Fish-hook” appearance in V4 | Yes | No |
NB. These features have limited specificity, therefore it may not always be possible to tell the difference between these two conditions.
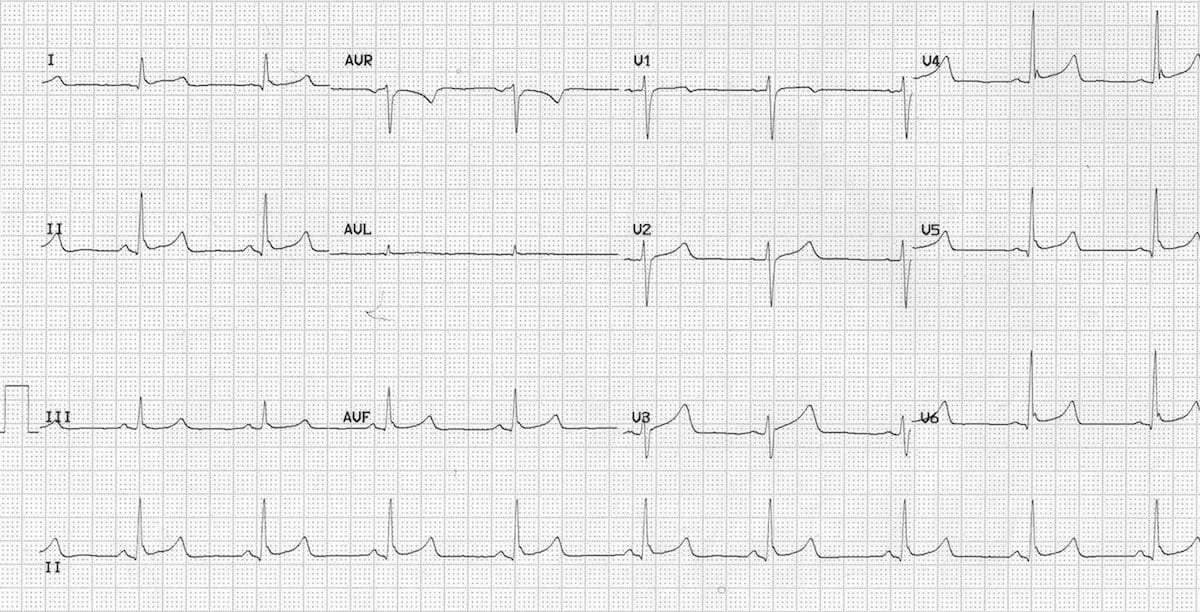
Look at this ECG example:
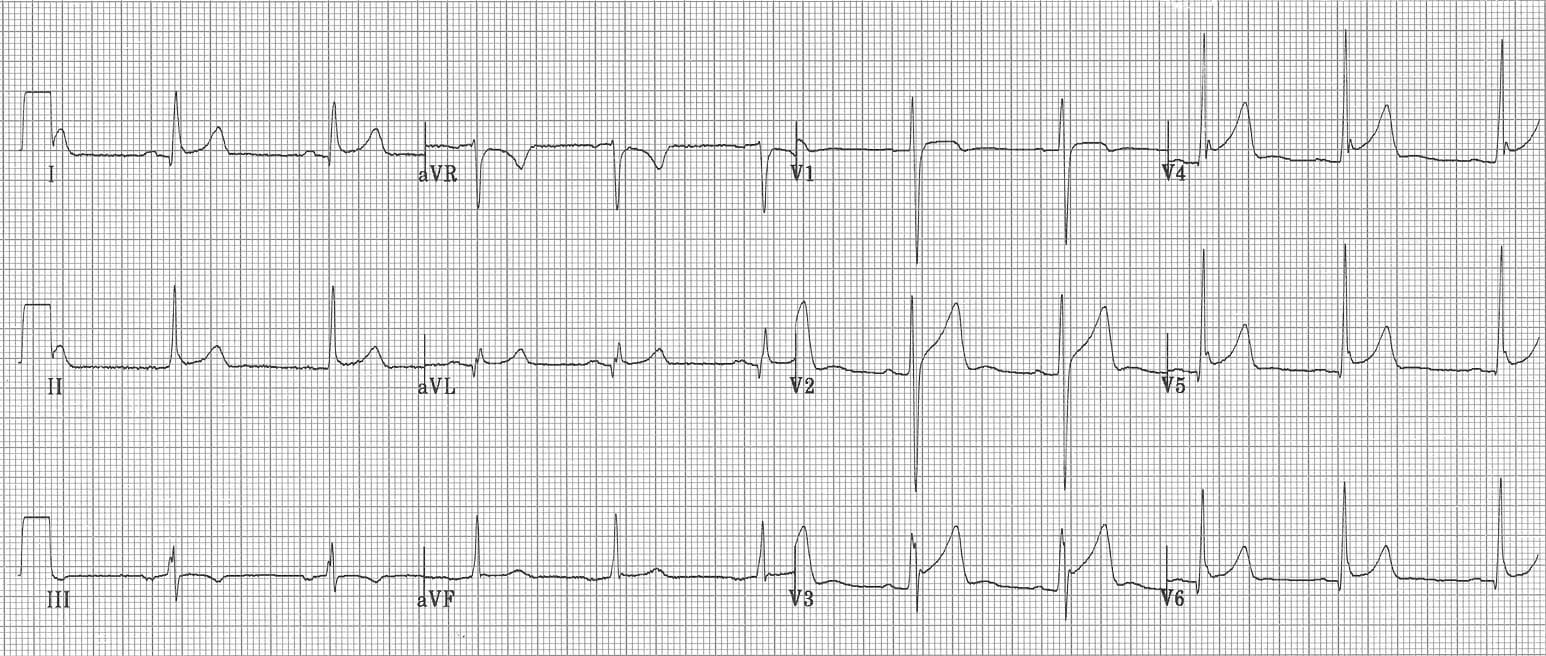
Is this BER or pericarditis?
Reveal Answer
There are features suggestive of pericarditis:
- Widespread concave ST elevation
- Subtle downsloping PR depression in limb (I, aVL) and precordial (V3-6) leads
- Subtle PR elevation in aVR
But also features suggestive of BER:
- ST elevation is markedly more prominent in precordial leads (especially V2-5)
- J-wave notching with fish-hook pattern in V3-4
- Prominent precordial T waves
- ST / T wave ratio of 0.16
These ECG appearances could be caused by BER alone, although it is possible that this ECG represents BER with superimposed pericarditis. This ECG demonstrates the difficulty in differentiating between these two very similar conditions.
Remember that it is possible for a patient with BER to get pericarditis!
Examples of BER
This ECG example was originally featured on the EMS-1.com website.
This ECG was originally featured on Dr Smith’s ECG Blog. and discussed in the video below: ‘Inferior ST Elevation: what is the Diagnosis?‘
Not So “Benign”?
Initially introduced as a benign ECG pattern, subsequent literature has raised links between early repolarisation patterns and sudden cardiac death:
- A 2008 study found a higher incidence of BER patterns among patients resuscitated following idiopathic VF arrest (OR 10.9). These patterns were present on pre-morbid ECGs.
- A large Finnish cohort study published in NEJM Dec 2009 found that an early-repolarization pattern in the inferior leads was associated with an increased risk of death from cardiac causes in middle-aged subjects over a 30-year follow-up period.
- The difficulty lies in discerning which patients are at risk of these events, as BER is prevalent in healthy young individuals (3-5%) whom which do not suffer adverse events
- Early Repolarisation Syndrome (ERS) refers to the presence of a BER ECG pattern in individuals resuscitated following arrest due to idiopathic VF. There is some literature suggesting global early repolarisation (compared with isolated lateral leads) gives a higher predisposition to onset or recurrence of idiopathic VF
Related Topics
- Pericarditis
- Interval: J-point
- Le Syndrome de Haïssaguerre (idiopathic VF)
References
- Edhouse J, Brady WJ, Morris F. ABC of clinical electrocardiography: Acute myocardial infarction-Part II. BMJ. 2002; 324: 963-6.
- Haïssaguerre M, Derval N, Sacher F, Jesel L, Deisenhofer I, de Roy L, et al. Sudden cardiac arrest associated with early repolarization. N Engl J Med. 2008 May 8;358(19):2016-23
- Tikkanen JT, Anttonen O, Junttila MJ, Aro AL, Kerola T, Rissanen HA, et al. Long-term outcome associated with early repolarization on electrocardiography. N Engl J Med. 2009 Dec 24;361(26):2529-37
- Grauer K. ECG Interpretation Review – #2 [“Smiley” ST, ST Elevation, Early Repolarization, LVH by Voltage]
- EMS 12-Lead‘s Tom Bouthillet explains BER with some great ECG examples.
- Dr Stephen Smith discusses some clever ways to distinguish between BER and acute ischaemia.
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
ECG LIBRARY
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.
Hi Ed. Your blog is excellent! But for the record, I believe it was me to popularize the “smiley” vs “frowny”-shape ST segments, in my 1st ECG publication back in 1983. I’ve taught this finding ever since — 🙂 Ken Grauer ([email protected]) — That said, keep up the GREAT work with your web site !!!
Thanks Ken, have attributed accordingly, and found a quote from the old days…
Hello,
I have a question on the “notch” in Benign Early Repolarization (BER). Why is it that the “notch” BER is usually regarded as the small peak/upward deflection near the end of the S wave? A notch is supposed to be a small indentation, cleft, groove, nick, or downward deflection, rather than an upward deflection (bump). A notch shouldn’t be a bump pointing upwards but a small indentation pointing downwards. Why is the definition of notching different when it comes to BER notching? I’d appreciate your thoughts.
Vick.