
![]()
ECG Case 002
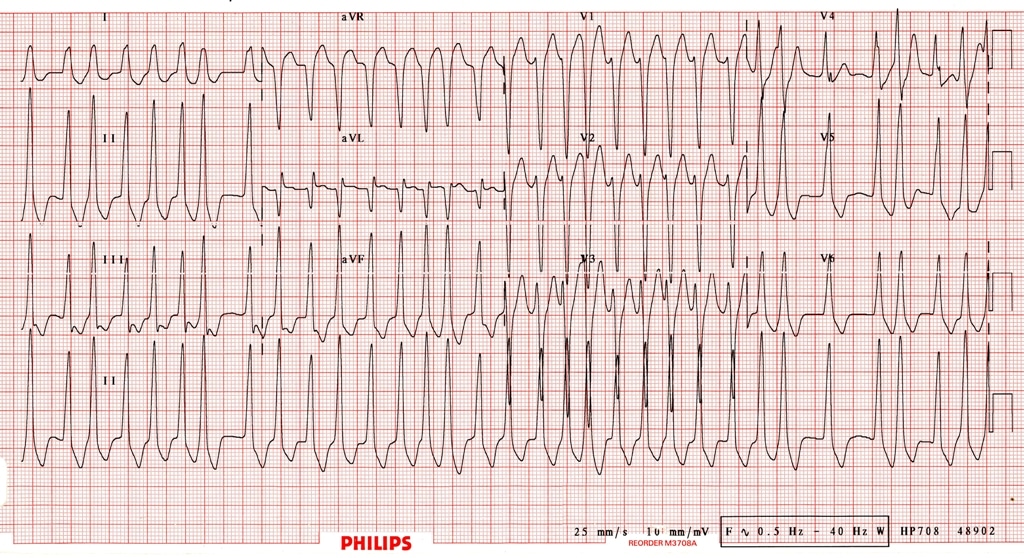
20-year old female presenting with palpitations and presyncope, BP 75/50
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
Main Abnormalities:
- Irregularly irregular broad complex tachycardia
- Extremely rapid ventricular rates — up to 300 bpm in places (RR intervals as short as 200ms or 1 large square)
- Beat-to-beat variability in the QRS morphology, with subtle variation in QRS width
Explanation of ECG Findings:
- Irregularly irregular rhythm is consistent with atrial fibrillation
- There is a left bundle branch block morphology to the QRS complexes
- However, the ventricular rate is far too rapid for this to be simply AF with LBBB
- The rates of 250-300 bpm and the variability in QRS complex morphology indicate the existence of an accessory pathway between the atria and ventricles
Diagnosis:
- These findings indicate atrial fibrillation in the context of Wolff-Parkinson-White syndrome
CLINICAL PEARLS
- Broad complex irregular tachycardia at very rapid rates? -> Suspect AF with WPW!
- These patients can rapidly become haemodynamically unstable
- The options for chemical cardioversion are very limited, favouring DC cardioversion
We would recommend immediate DC cardioversion in this patient. Our approach would be:
- Fluid load with 0.5 – 1L crystalloid bolus
- Add in a push-dose vasopressor to elevate the BP (e.g. Metaraminol 0.5 – 1mg IV)
- Sedate with something that has minimal effects on BP (e.g. fentanyl or ketamine in cautious doses)
- Shock at 200J biphasic. Consider using an AP pad position for maximal 1st shock success
References
Further Reading
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
TOP 100 ECG Series
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.
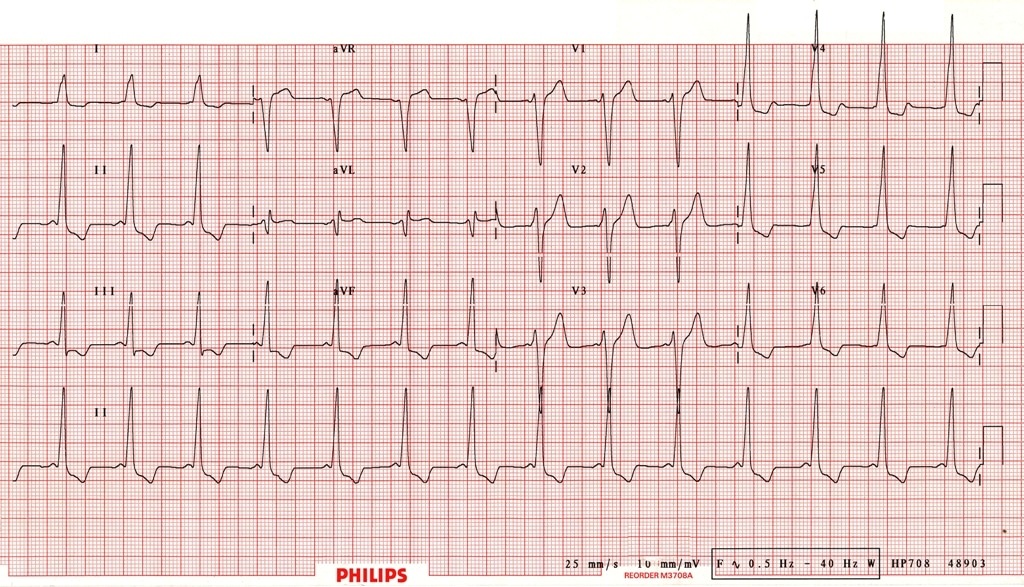
Hi guys, I’m a cardiologist and want to congratulate you on this outstanding library of ECGs. One of our registrar’s “borrowed” the ECG from this case (002) as an example of pre-excited AF and my ears pricked up a little….the pedant in me isn’t convinced that this is what it seems. Unless you can post the ECG in SR showing a superoparaseptal AP, I have a feeling this may be an irregular RVOTVT…..I could be wrong.
The QRS forces in the majority of beats are very rapid and have no real slurring from initial muscular conduction. In addition, the negative QS in aVL is unusual (but not impossible) for these pathways. Lastly, do I see negative P waves in leads 3 and aVF?
As I say, your site is first class and a wonderful teaching tool. It has become a boon for those wishing to include high quality 12 leads in talks and presentations so when you go “public”, clearly you’ve got to be 100% accurate and I have some sneaky doubts on this one. Hope I’m wrong!
BW
thank you for your wonderful ecg pool.They are fabulous
Can you please clarify why this would be AF with WPW and not a VT?
I am confused too
I am a student also I thought it is a VT , but the RR interval is irregularly irregular , and the q wave is kinda hidden- like the delta wave – so I suspected WPW – but I also leaned toward the diagnosis of VT
I seriously thought this was vt🥲