
![]()
ECG Case 137
55-year-old woman presenting with exertional crushing chest pain, worsening over recent days. The monitor alarms “extreme tachycardia” — a rhythm strip is recorded:

Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
At first glance, broad complexes varying in duration and amplitude may appear to represent polymorphic ventricular tachycardia (VT).
However, on closer inspection we note three features that suggest this is artefact:
- The onset is too abrupt, and there is no ‘R-on-T’ phenomenon — the apparent tachycardia begins after a T wave. Polymorphic VT is usually initiated by a premature ventricular complex (PVC) or premature atrial complex (PAC) that ‘lands’ on the preceding T wave
- The rate in the initial portion of the rhythm strip is simply too high for VT — if you look closely it is approaching 600 bpm
- Lastly, we can see QRS complexes ‘marching’ through at a rate of 60 bpm (every 5 large squares)
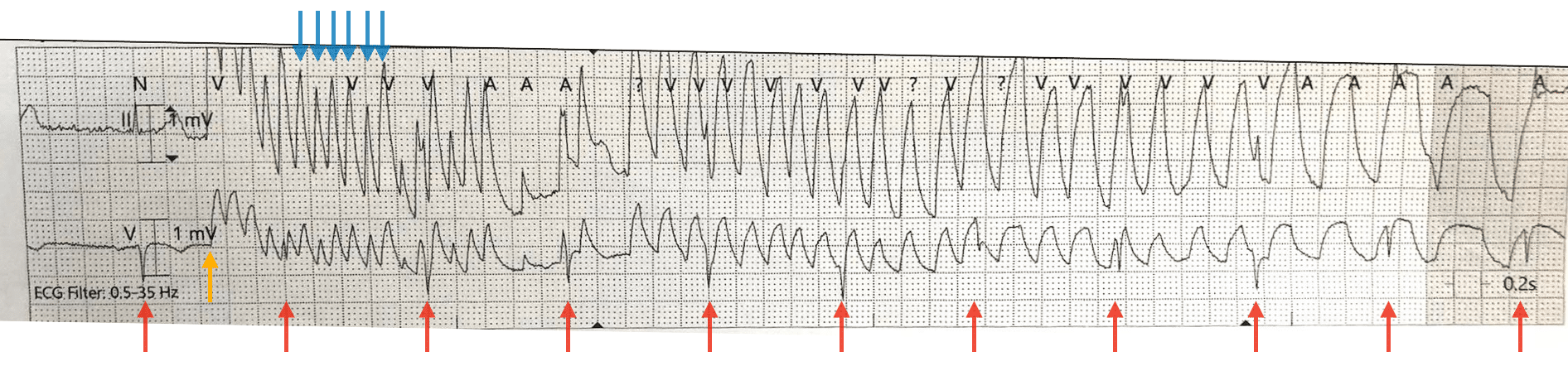
Blue: Apparent ventricular rate approaching 600 bpm
Red: QRS complexes ‘marching’ through at 60 bpm
Most importantly, the patient was still conscious and had no change in symptoms!
Let’s compare the above example to a true case of polymorphic VT:

- There are frequent PVCs after the second, third and fourth QRS complexes. The fourth PVC lands on the preceding T wave (‘R on T’ phenomenon), triggering a run of polymorphic VT
- The rate is regular at approximately 300 bpm
- Note subsequent degeneration into ventricular fibrillation (VF)
CLINICAL PEARLS
Alarms and calls for ‘VTach’ are common for pre-hospital, emergency, and ward-based clinicians.
Artefacts generated by voluntary or involuntary movements during an ECG recording can simulate malignant arrhythmias and lead to unnecessary interventions. On the contrary, mistaking a true arrhythmia for artefact can have dire consequences.
Firstly, look at the patient. If there is no change to the clinical picture, take a closer look at the rhythm strip. An atypical onset, extremely high rates, and QRS complexes “marching” through may suggest artefact.
The presence of an unchanged pulse oximetry curve further points towards the presence of artefact.
Further reading
Related topics
References
- Longo et al. Ventricular tachycardia or artifact? Journal of Thoracic Disease 2018 Mar; 10(3): 2046-2047
TOP 150 ECG Series

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.

Interventional cardiologist, ECG and hemodynamics fan. MD, Assoc. Prof. at Marmara University, Pendik T&R Hospital, Assoc. Editor at Archives of TSC, ESC National Prevention Coordinator