
![]()
Premature Ventricular Complex (PVC)
A premature ventricular complex (PVC) is a premature beat arising from an ectopic focus within the ventricles. AKA: ventricular ectopics, ventricular extrasystoles, ventricular premature beats, ventricular premature depolarisations.
ECG features of PVCs
- Broad QRS complex (≥ 120 ms) with abnormal morphology
- Premature — i.e. occurs earlier than would be expected for the next sinus impulse
- Discordant ST segment and T wave changes.
- Usually followed by a full compensatory pause
- Retrograde capture of the atria may or may not occur
Origin of Ectopic Beats
- Groups of pacemaker cells throughout the conducting system are capable of spontaneous depolarisation
- The rate of depolarisation decreases from top to bottom: fastest at the sinoatrial node; slowest within the ventricles
- Ectopic impulses from subsidiary pacemakers are normally suppressed by more rapid impulses from above
- However, if an ectopic focus depolarises early enough — prior to the arrival of the next sinus impulse — it may “capture” the ventricles, producing a premature contraction
- Premature contractions (“ectopics”) are classified by their origin — atrial (PACs), junctional (PJCs) or ventricular (PVCs)
Electrophysiology of Ventricular Ectopics
- Ectopic firing of a focus within the ventricles bypasses the His-Purkinje system and depolarises the ventricles directly
- This disrupts the normal sequence of cardiac activation, leading to asynchronous activation of the two ventricles
- The consequent interventricular conduction delay produces QRS complexes with prolonged duration and abnormal morphology
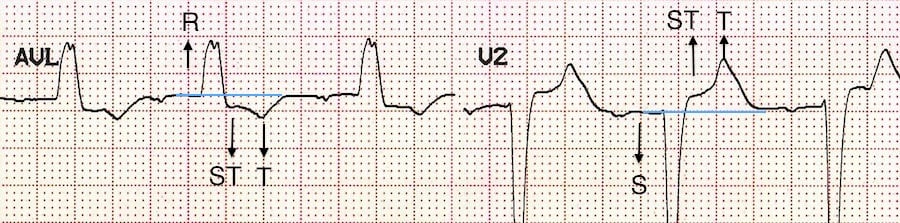
Discordance
Appropriate discordance describes a pattern of repolarisation abnormality (typically seen with left bundle branch block, paced rhythms, VT) in which the ST segment and T wave are directed opposite to the main vector of the QRS complex. Because there is abnormal depolarisation, there is subsequent abnormal repolarisation which is discordant:
- ST depression and T wave inversion in leads with a dominant R wave
- ST elevation with upright T waves in leads with a dominant S wave
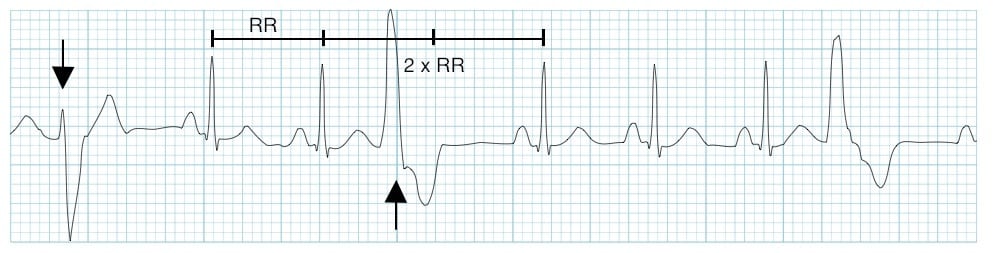
With a full compensatory pause, the next normal beat arrives after an interval that is equal to double the preceding R-R interval
Retrograde capture describes the process whereby the ectopic impulse is conducted retrogradely through the AV node, producing atrial depolarisation. This is visible on the ECG as an inverted P wave (“retrograde P wave“), usually occurring after the QRS complex.
PVCs are said to be “frequent” if there are more than 5 PVCs per minute on the routine ECG, or more than 10-30 per hour during ambulatory monitoring.
Classification
PVCs may be either:
- Unifocal — arising from a single ectopic focus; each PVC is identical
- Multifocal — arising from two or more ectopic foci; multiple QRS morphologies
The origin of each PVC can be discerned from the QRS morphology:
- PVCs arising from the right ventricle have a left bundle branch block morphology (dominant S wave in V1)
- PVCs arising from the left ventricle have a right bundle branch block morphology (dominant R wave in V1)
PVCs often occur in repeating patterns:
- Bigeminy — every other beat is a PVC
- Trigeminy — every third beat is a PVC
- Quadrigeminy — every fourth beat is a PVC
- Couplet — two consecutive PVCs
- NSVT — between three and thirty consecutive PVCs (see below)
Clinical Significance
- PVCs are a normal electrophysiological phenomenon not usually requiring investigation or treatment
- Frequent PVCs may cause palpitations and a sense of the heart “skipping a beat”
- In patients with underlying predispositions (e.g. ischaemic heart disease, WPW), a PVC may trigger the onset of a re-entrant tachydysrhythmia — e.g. VT, AVNRT, AVRT
Frequent PVCs are usually benign, except in the context of an prolonged QTc, when they may predispose to malignant ventricular arrhythmias such as Torsades de Pointes by causing “R on T” phenomenon
Causes
Frequent or symptomatic PVCs may be due to:
- Anxiety
- Sympathomimetics
- Beta-agonists
- Excess caffeine
- Hypokalaemia
- Hypomagnesaemia
- Digoxin toxicity
- Myocardial ischemia
Example ECGs
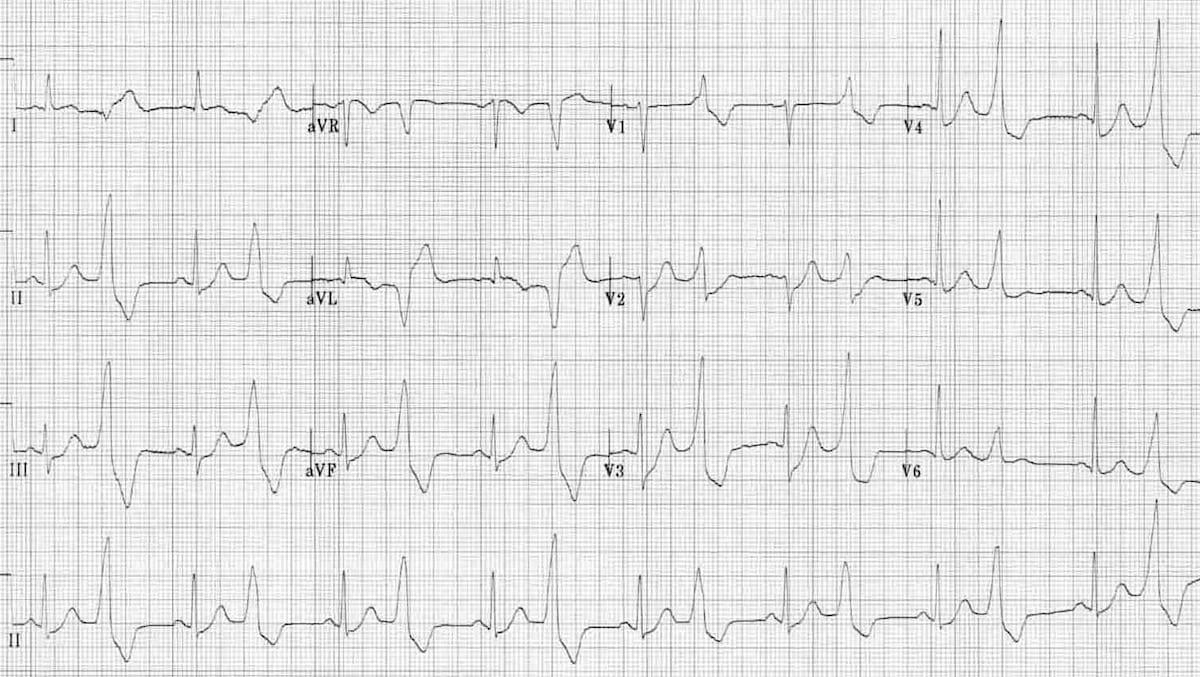
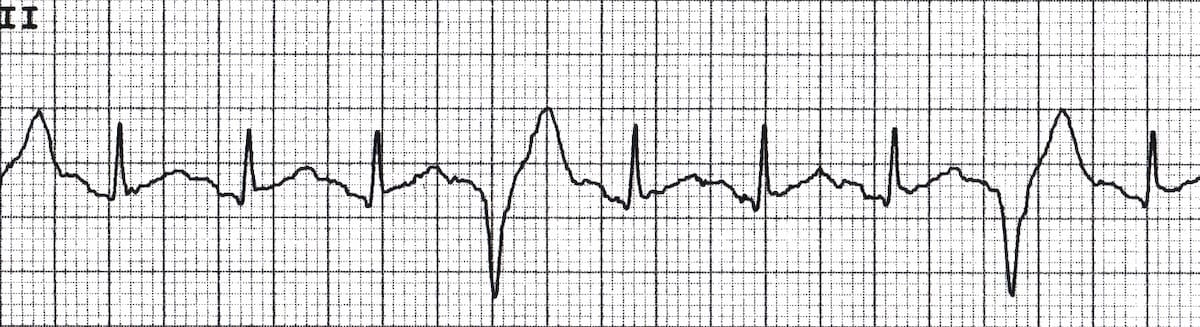
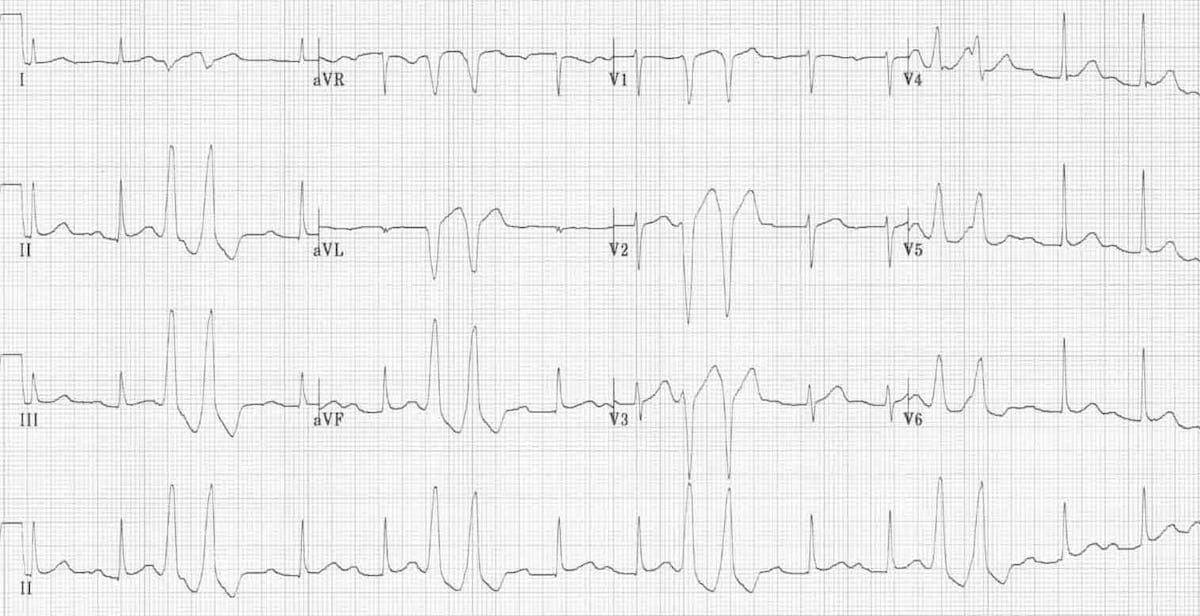
Multifocal PVCs
- Sinus rhythm with PVCs of two different morphologies (arrows)
- Note the appropriately discordant ST segments / T waves
- The pause surrounding the PVC is equal to double the preceding R-R interval (= a full compensatory pause)
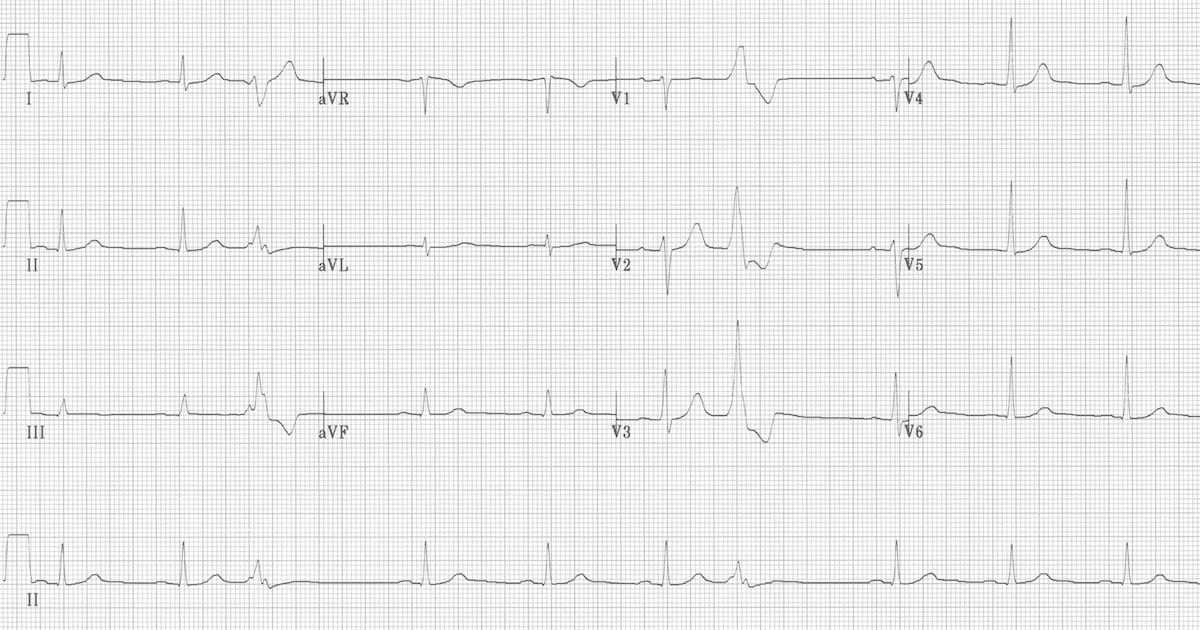
Ventricular bigeminy

Ventricular quadrigeminy
PVC pairs (couplets)
Non-sustained VT (NSVT)

When is a PVC not a PVC?
- Definitions vary regarding 3 or more PVCs
- Some authors define three PVCs as a triplet of PVCs; whilst others describe this as a ‘short burst of VT’; but more commonly as NSVT
- A consensus definition would be: 3-30 consecutive PVCs with a rate >100bpm described as non-sustained VT (ventricular rhythm if rate <100bpm)
Learn from the experts
Related Topics
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
ECG LIBRARY
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.

Hi there silly question time 🙂
Within the hospital setting where i work there is varying answers when it comes to recording Ventricular Bigeminy for nurses whilst attending to bedside observations.
What is the best way to record- the peripheral pulse rate felt or the telemetry rate captured ?
A patient with a telemetry rate of 80 found with pulse rate of 38, therefore requires a clinical review by the nurses but often told to just record the telemetry rate. Is a patient with ventricular Bigeminy with a peripheral pulse rate of 38 at risk of hypoperfusion as only contracting at a rate of 38 as a PVC is not an actual full contraction by the heart?
The nurse should also take into consideration a full clinical picture and whether a patient is symptomatic or not.
Thanks Sharon