
![]()
Premature Atrial Complex (PAC)
A premature atrial complex (PAC) is a premature beat arising from ectopic pacemaking tissue within the atria. There is an abnormal P wave, usually followed by a normal QRS complex. AKA: Atrial ectopics, atrial extrasystoles, atrial premature beats, atrial premature depolarisations.
ECG features of PACs
- Abnormal (non-sinus) P wave usually followed by a normal QRS complex (< 120 ms)
- Post-extrasystolic pauses may be present — PACs that reach the SA node may depolarise it, causing the SA node to be “reset”, with a longer-than-normal interval before the next sinus beat arrives
- PACs may also be conducted aberrantly (usually RBBB morphology), or not conducted at all. P waves will still be visible in both cases
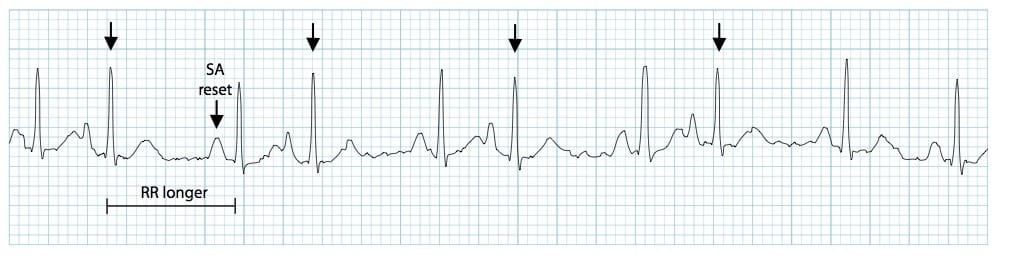
- Unlike with a premature ventricular complexe (PVC), the post-extrasystolic pause is not equal to double the preceding RR interval
P wave morphology
- The P wave typically has a different morphology and axis to the sinus P waves
- PACs arising close to the AV node (“low atrial” ectopics) cause retrograde activation of the atria, producing an inverted P wave with a relatively short PR interval ≥ 120 ms (PR interval < 120 ms is classified as a PJC)
- The abnormal P wave may be hidden in the preceding T wave, producing a “peaked” or “camel hump” appearance — if this is not appreciated the PAC may be mistaken for a premature junctional complex (PJC)
Aberrancy and “blocked” PACs
- PACs arriving early in the cycle may be conducted aberrantly, usually with a RBBB morphology (as the right bundle branch has a longer refractory period than the left). They can be differentiated from PVCs by the presence of a preceding P wave
- Similarly, PACs arriving very early in the cycle may not be conducted to the ventricles at all. In this case, you will see an abnormal P wave that is not followed by a QRS complex (“blocked PAC”). It is usually followed by a compensatory pause as the sinus node resets
Origin of Ectopic Beats
- Groups of pacemaker cells throughout the conducting system are capable of spontaneous depolarisation
- The rate of depolarisation decreases from top to bottom: fastest at the sinoatrial node; slowest within the ventricles
- Ectopic impulses from subsidiary pacemakers are normally suppressed by more rapid impulses from above
- However, if an ectopic focus depolarises early enough — before the arrival of the next sinus impulse — it may “capture” the ventricles, producing a premature contraction
- Premature contractions (“ectopics”) are classified by their origin — atrial (PAC), junctional (PJC) or ventricular (PVC)
Classification of PACs
PACs may be either:
- Unifocal – arising from a single ectopic focus; each PAC is identical.
- Multifocal – arising from two or more ectopic foci; multiple P-wave morphologies.
PACs often occur in repeating patterns:
- Bigeminy — every other beat is a PAC
- Trigeminy — every third beat is a PAC
- Quadrigeminy — every fourth beat is a PAC
- Couplet – two consecutive PACs
- Triplet — three consecutive PACs
Clinical significance of PACs
- PACs are a normal electrophysiological phenomenon not usually requiring investigation or treatment
- Frequent PACs may cause palpitations and a sense of the heart “skipping a beat”
- In patients with underlying predispositions (e.g. left atrial enlargement, ischaemic heart disease, WPW), a PAC may be the trigger for the onset of a re-entry tachyarrhythmia — e.g. Atrial fibrillation, atrial flutter, AVNRT, AVRT
Causes of PACs
Frequent or symptomatic PACs may occur due to:
- Anxiety
- Sympathomimetics
- Beta-agonists
- Excess caffeine
- Hypokalaemia
- Hypomagnesaemia
- Digoxin toxicity
- Myocardial ischaemia
ECG Examples
Example 1

Blocked PAC:
- This hidden PAC gives a peaked appearance to the T wave (circled)
- The PAC is not not followed by a QRS complex, indicating that it has not been conducted to the ventricles (“blocked PAC”)
- It is followed by a compensatory pause
Example 2
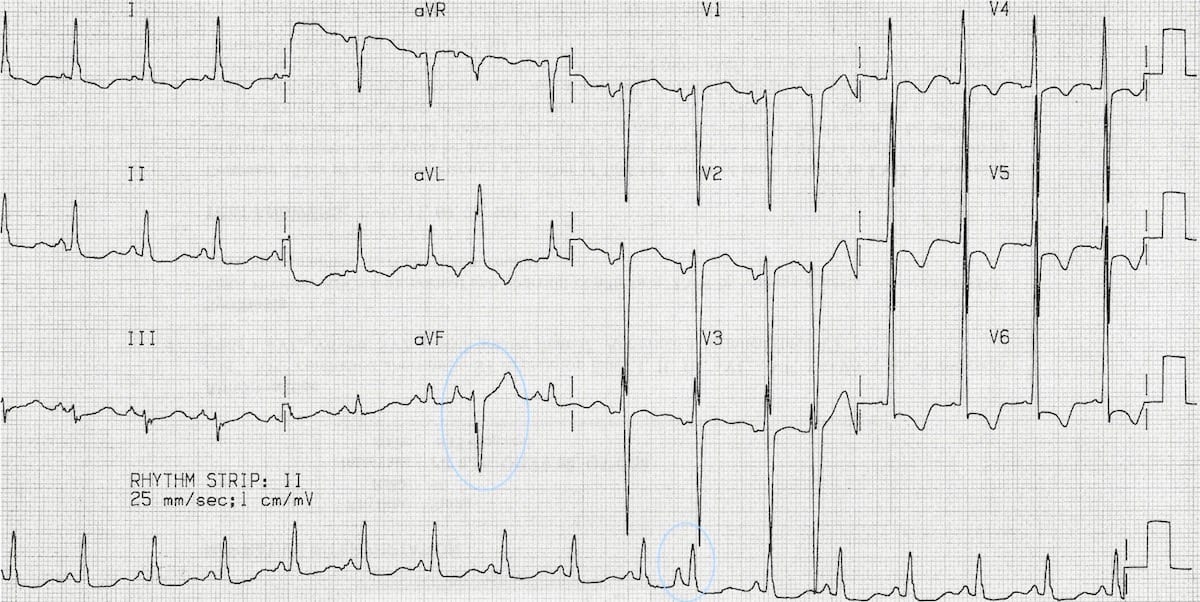
Normally and aberrantly-conducted PACs:
- There is an aberrantly conducted PAC, best seen in aVL and aVF (circled)
- This could be mistaken for a ventricular ectopic — however, it is clearly preceded by an abnormal P wave
- A normally-conducted PAC is also present on the rhythm strip (circled)
NB: This rhythm strip is not recorded simultaneously
Related Topics
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
ECG LIBRARY
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.