
![]()
History of Neuraxial Anaesthesia
Neuraxial anaesthesia (neuraxial blockade) refers to local anaesthetic techniques delivered around the spinal cord and nerve roots, principally spinal anaesthesia (intrathecal/subarachnoid) and epidural anaesthesia (extradural/peridural, including caudal). Modern practice relies on distinct confirmation endpoints: intrathecal placement is confirmed by free cerebrospinal fluid (CSF) flow, whereas epidural placement is inferred from loss-of-resistance and related indirect signs (including hanging-drop and pressure-based methods).
Historically, neuraxial techniques advanced alongside innovations in needle design, catheter placement, and reproducible methods for identifying anatomical planes. The eponym landscape reflects this. Some terms remain precise (e.g. Quincke and lumbar puncture), while others have drifted into generic usage (e.g. “Tuohy” often used as shorthand for many epidural needle designs despite later modification and variation).
Clinically, neuraxial blockade remains central to obstetrics, perioperative analgesia, and pain medicine. Its evolution is a recurring story of practical problems such as block reliability, post-dural puncture headache (PDPH), catheter direction and dosing control. These drive successive solutions from early caudal injections to continuous catheter epidurals and directional needle tips designed to guide catheters.
Neuraxial blockade timeline
Foundations that made neuraxial blockade possible
1844 – Francis Rynd introduces hypodermic (subcutaneous) perineural morphine instillation for neuralgia at the Meath Hospital in May 1844. A practical precursor to regional injection-based analgesia. He later provided a formal description of his instrument in (1861).
On the 13th of November [1844] the fluid was introduced, ten grains acetate morphia to the drachm of creosote, one punture behind the trochanter, and one half-way down the thigh. He was instantly relieved from pain, and walked steadily through the ward without any pain or difficulty
Rynd, 1845
1853 – Development of syringe and hollow needle technology. Charles Gabriel Pravaz (1791–1853) described a screw-driven syringe with a fine trocar for intravascular injection of ferric chloride into naevi (published in 1853). Alexander Wood performed therapeutic injections and published (1855) the first widely reproducible clinical account of hypodermic morphine for neuralgia.
On November 28th [1853] I attended an old lady, who had suffered severely for four days from cervico-brachial neuralgia…I inserted the syringe within the angle formed by the clavicle and acromion, and injected twenty drops of a solution of muriate of morphia…in half an hour the pain had subsided, and I left her in the anticipation of a refreshing sleep.
Wood, 1855
1884 – Cocaine becomes the first practical local anaesthetic in clinical use. Ophthalmologist Carl Koller (1857–1944) introduces cocaine as the first practical local anaesthetic for clinical use. Koller’s clinical demonstration of topical cocaine in ophthalmology triggered rapid uptake of injection-based regional techniques, underpinning subsequent experiments in nerve block and early neuraxial cocaine injection work.
First neuraxial drug experiments
1885 – James Leonard Corning (1855–1923) conducted a series of experiments injecting hydrochlorate of cocaine between the lumbar spinous processes in dogs and later in a human subject. He observed segmental sensory changes and motor effects in the lower limbs, publishing his findings in Spinal anaesthesia and local medication of the cord. These experiments constitute the first published description of the principle of neuraxial blockade. Long regarded as “first spinal blockade”, but later reviews consider the injection intrathecal and likely extradural.
Spinal anaesthesia and CSF access
1891 – Heinrich Irenäus Quincke (1842–1922) is credited with the development and standardisation of lumbar puncture as a repeatable, minimally invasive method for CSF pressure relief and fluid sampling. Diagnostic lumbar puncture becomes the technical gateway for intrathecal anaesthesia. The “Quincke needle” becomes archetypal cutting bevel needle for neuraxial access.
The fluid was withdrawn via a fine needle between the third and fourth lumbar vertebrae. Pressure readings were taken before and after drainage… and samples analysed for protein, sugar, cells, and bacteria.
Quincke 1891
1891 – In parallel, Walter Essex Wynter (1860-1945) attempts therapeutic CSF pressure relief in paediatric meningitis via incision-based thecal puncture and drainage tubing, a more surgical decompression approach than Quincke’s needle puncture.
1898 – On August 16, August Bier performed the first spinal anaesthetic using cocaine on a 34 year old man undergoing a partial amputation of the leg. His vivid description of post-dural puncture headache (PDPH) becomes a key driver for later needle refinement.
1900 – Oskar Kreis (1872-1958) applies spinal anaesthesia to obstetrics (labour and operative delivery). In Über Medullarnarkose bei Gebärenden Kreis demonstrates the feasibility of spinal (subarachnoid) cocaine analgesia feasibility and highlights the burden of side effects in early intrathecal practice.
Epidural and caudal routes
1901 – Jean-Athanase Sicard and Fernand Cathelin independently describe caudal epidural injection via the sacral hiatus “dans le canal sacré, en dehors des méninges”. Initially used for minor durgical and urological operations.
1909 – Walter Stoekel introduces caudal epidural for labour pain relief. He publishes Über sakrale Anästhesie detailing 141 cases of obstetric epidural analgesia via the caudal route, the first large obstetric series of caudal (sacral) epidural analgesia.
Lumbar epidural “metameric” era
1921 – Fidel Pagés publishes Anestesia Metamérica, the first clear clinical description of thoracolumbar epidural (“metameric”) anaesthesia with segmental blockade in humans. One of the earliest clear presentations of epidural anaesthesia as a surgical technique distinct from spinal anaesthesia
1922 – Sicard and Jacques Forestier introduce intrathecal lipiodol myelography, demonstrating contrast mapping of the subarachnoid space for neuraxial diagnosis rather than analgesia.
1931 – Eugen Bogdan Aburel describes one of the earliest continuous peridural catheter techniques for obstetric analgesia, linking neuraxial blockade to repeat dosing through an indwelling catheter.
1931 – Achille Mario Dogliotti further develops lumbar epidural anaesthesia and popularises the loss-of-resistance (LOR) approach as a reproducible way to identify the epidural space.
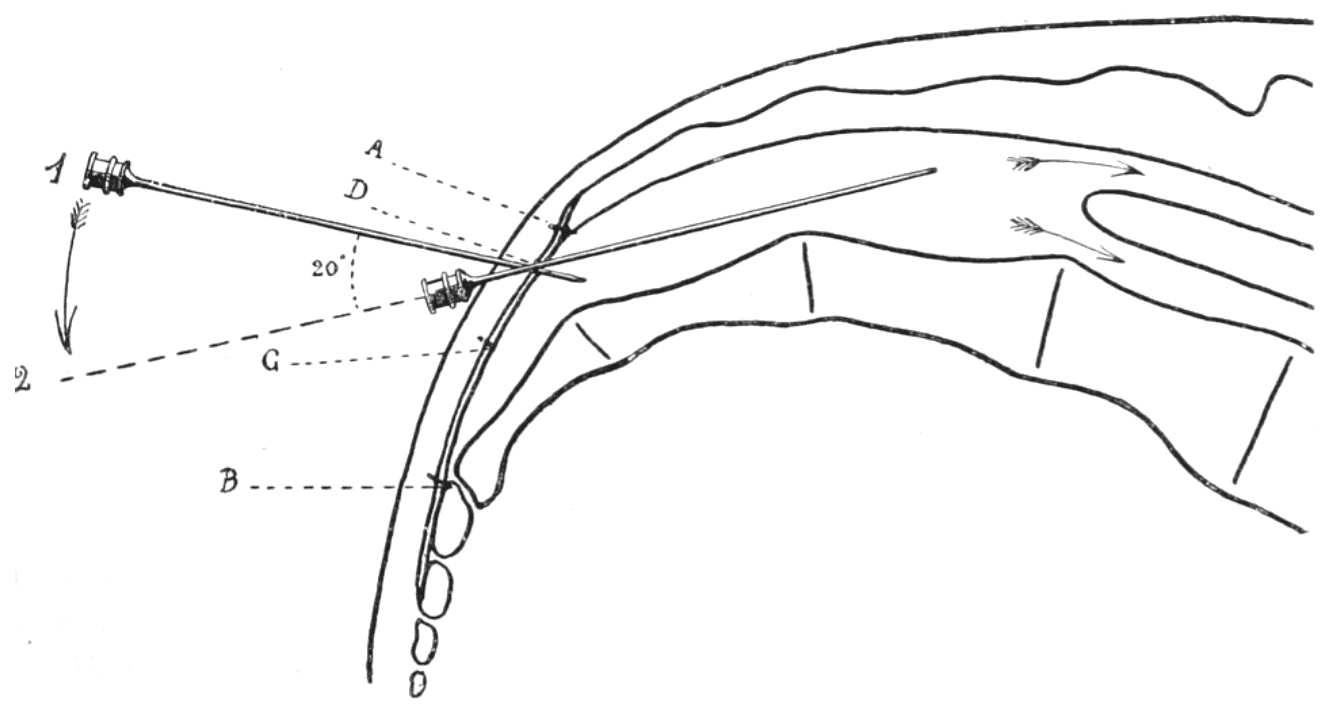
1932 – Angelo Luigi Soresi described a method of injecting anaesthetic fluid into the peridural (epidural) space, obtaining the same anesthetic results of spinal anesthesia without its unpleasant features. His hanging drop technique of locating the epidural space was developed independent of Gutiérrez
The surgeon watches carefully the fluid in the shank of the needle while pushing very slowly the needle toward the spine. Suddenly it will be noticed that the fluid disappears from the shank, as if it had been sucked away. This phenomenon indicates that the needle has entered the epidural space.
Soresi 1932
1933 – Alberto Gutiérrez describes his hanging drop sign (gota colgante) as a visual method for identifying entry into the epidural space. A drop of local anaesthetic (or saline) is placed at the hub of an epidural needle. As the needle advances, the drop is aspirated into the needle when the tip enters the epidural space due to negative pressure and tissue recoil.
Continuous neuraxial techniques and catheter era
1940 – William Thomas Lemmon demonstrates continuous spinal anaesthesia by maintaining access to the subarachnoid space using a malleable spinal needle left in situ, allowing repeated administration of small doses of local anaesthetic. However, the technique remained technically complex, required specialised equipment (a Lemmon mattress), and carried risks related to prolonged intrathecal needle placement.
1941 – Robert Andrew Hingson and Waldo Edwards popularise continuous caudal analgesia in obstetrics. They develop the Hingson–Edwards malleable caudal needle for prolonged access to the epidural space for titratable dosing over hours.
1942 – Hingson and James L. Southworth attempt continuous lumbar peridural anaesthesia. Hardware limitations with large needles and catheters, reinforced the need for directional epidural needle designs.
1943 – Ralph Huber develops and patents (1946) the Huber point epidural needle. A non coring needle with a transversely curved wall and side hole giving it a long, sharp, curved tip.
1945 – Edward Boyce Tuohy developed a needle with a Huber-type curved point and side orifice for the placement of spinal and epidural catheters. Tuohy published before Huber’s 1946 patent became widely known, and the needle subsequently entered anaesthetic practice under the name “Tuohy needle”.
1947 – Pío Manuel Martínez Curbelo performs the first described lumbar epidural catheter placement on January 13, 1947 and publishes the method in 1949, cementing the transition to continuous lumbar epidural anaesthesia.
Modern consolidation
1954 – Philip Raikes Bromage textbook era: epidural anaesthesia enters modern standardisation and teaching frameworks.
1979 – Epidural opioids enter the modern pain era (Behar et al.), expanding neuraxial practice beyond local anaesthetic blockade.
Modern era – Neuraxial practice defined by distinct confirmation endpoints (CSF flow vs indirect epidural signs), with adjuncts (pressure waveform/ultrasound) where needed.
Key contributors
- Francis Rynd (1801-1861), Irish surgeon — first documented subcutaneous (hypodermic) morphine injection for neuralgia (1844/1845).
- Alexander Wood (1817-1884), Scottish physician — popularised hypodermic morphine injection as a reproducible clinical method (1855).
- Carl (Karl) Koller (1857–1944), Austrian ophthalmologist — introduced cocaine as the first practical local anaesthetic (1884).
- James Leonard Corning (1855–1923), American neurologist — first published neuraxial cocaine injection experiments (likely epidural), establishing neuraxial blockade concept (1885).
- Heinrich Irenäus Quincke (1842-1922), German physician — introduced and standardised lumbar puncture for CSF pressure relief and sampling (1891).
- Walter Essex Wynter (1860-1945), English physician — incision-based lumbar thecal puncture and continuous CSF drainage for meningitis “cerebral pressure” (1889–1891).
- August Karl Gustav Bier (1861-1949), German Surgeon — first widely accepted surgical spinal anaesthesia (intrathecal cocaine) (1898).
- Oskar Kreis (1872-1958), Swiss obstetrician–gynaecologist — early obstetric spinal anaesthesia/analgesia (1900).
- Jean-Athanase Sicard (1872–1929), French physician — caudal epidural injections (1901) and intrathecal lipiodol myelography with Forestier (1921–1922).
- Fernand Cathelin (1873–1929), French physician — independent pioneer of caudal epidural injection (1901); systematised the method (1903).
- Walter Stoeckel (1871–1961), German obstetrician–gynaecologist — large-series caudal epidural analgesia in labour (1909).
- Fidel Pagés Miravé (1886–1923), Spanish military surgeon — “Anestesia metamérica”, first clear thoracolumbar epidural anaesthesia description (1921).
- Achille Mario Dogliotti (1897–1966), Italian surgeon — disseminated lumbar epidural technique; popularised loss-of-resistance / saline syringe localisation (1932–1933).
- Eugen Bogdan Aburel (1899–1975), Romanian obstetrician and gynecologic surgeon — early continuous peridural (catheter) analgesia in obstetrics (1931).
- Angelo Luigi Soresi (1877-1951), Italian-American surgeon — peridural anaesthesia report describing an early “drop disappears” localisation endpoint (1932).
- Alberto Gutiérrez (1892-1945), Argentine surgeon — “hanging drop” sign (gota colgante) for epidural space identification (1933).
- William Thomas Lemmon (1896-1974), American surgeon — continuous spinal anaesthesia systems (needle/catheter apparatus) (1940).
- Robert A. Hingson (1913–1996), American anesthesiologist — popularised continuous caudal analgesia in obstetrics (1941–1943).
- Ralph Lee Huber (1889-1953), American Dentist. — developed the Huber-point (non-coring) needle tip later used in directional neuraxial needles (1940s).
- Edward Boyce Tuohy (1908-1959), American anaesthesiologist — directional epidural needle for catheter techniques (mid-1940s).
- Pío Manuel Martínez Curbelo (1906-1962), Cuban anaesthesiologist — first described continuous lumbar epidural using a ureteral catheter via a directional needle (1947; published 1949).
References
Historical references
- Rynd F. Neuralgia – introduction of fluid to the nerve. Dublin Med Press 1845; 13: 167–168
- Rynd F. Description of an Instrument for the Subcutaneous Introduction of Fluids in Affections of the Nerves. Dublin Quarterly Journal of Medical Science. 1861; 32: 13
- Wood A. New method of treating neuralgia by the direct application of opiates to the painful points. Edinburgh Medical and Surgical Journal 1855; 82: 265-281
- Koller C. Ueber die Verwendung des Cocain zur Anästhesirung am Auge. Wiener medizinische Wochenschrift 1884; 43:1276-1277; 44:1310-1311
- Corning JL. Spinal anaesthesia and local medication of the cord. New York Medical Journal 1885; 42: 483-485
- Quincke HI. Ueber hydrocephalus. Verhandlungen des Congresses für Innere Medicin, Zehnter Congress, Gehalten zu Wiesbaden, vom 6.-9. April 1891: 321-339.
- Wynter WE. Four cases of tubercular meningitis in which paracentesis was performed for the relief of fluid pressure. Lancet 1891; 137(3531): 981-982
- Quincke HI. Die lumbalpunction des hydrocephalus. Berliner Klinische Wochenschrift 1891; 28: 929-933 and 965-968
- Bier A. Versuche über Cocainisirung des Rückenmarkes. Deutsche Zeitschrift für Chirurgie 1899; 51: 361. [Translated: Experiments Regarding the Cocainization of the Spinal Cord. Survey of Anesthesiology 1962; 6: 352–358]
- Kreis O. Über Medullarnarkose bei Gebärenden. Zentralblatt für Gynäkologie 1900; 24(28): 724–729.
- Sicard A. Les injections médicamenteuses extra-durales par voie sacrococcygienne. Comptes rendus des séances de la Société de biologie et de ses filiales. 1901; 53: 396-398.
- Cathelin F. Une nouvelle voie d’injection rachidienne. Méthode des injections épidurales par le procédé du canal sacré. Applications a l’homme. Comptes rendus des séances de la Société de biologie et de ses filiales 1901; 53: 452–453
- Stoeckel W. Über sakrale Anästhesie. Zentralblatt für Gynäkologie. 1909; 33: 1–15.
- Pagés F. Anestesia metamérica. Revista de sanidad militar (Madrid) 1921; 11(12): 351-365, 385-396
- Forestier J. Le trou de conjugasion vertébral et l’espace épidural. Étude anatomique et clinique. Essai de pathologie de l’espace épidural. 1922
- Aburel E. L’anesthésie locale continue (prolongée) en obstétrique. Bulletin de la Société d’obstétrique et de gynécologie de Paris. 1931; 20: 35-39.
- Dogliotti AM. Un nuovo metodo di anestesia tronculare in studio. La rachianestesia peridurale segmentaria. Arch Ital Chir. 1932; 38: 797-800
- Dogliotti AM. A new method of block anesthesia. Segmental peridural spinal anesthesia. The American Journal of Surgery. 1933; 20: 107-119
- Gutiérrez A. Anestesia metamérica epidural. Revista de cirugía de Buenos Aires, 1932; 11: 665-682.
- Lemmon WT. A method for continuous spinal anesthesia: A preliminary report. Ann Surg. 1940 Jan;111(1):141-4
- Edwards WB, Hingson RA. Continuous Caudal Anesthesia During Labor and Delivery. Anesthesia & Analgesia: 1942; 21(6): 301-311
- Southworth JL, Hingson RA. Continuous Caudal Analgesia in Surgery. Ann Surg. 1943 Dec; 118(6): 945-970.
- Tuohy EB. Continuous Spinal Anesthesia: Its usefulness and technic involved. Anesthesiology 1944;5:142-148
- Tuohy EB. Continuous Spinal Anaesthesia: A new method utilizing a ureteral catheter. Surg clin North AM 1945;25:834-840
- Martínez Curbelo M. Continuous peridural segmental anesthesia by means of a ureteral catheter. Curr Res Anesth Analg. 1949 Jan-Feb;28(1):13-23
- Bromage PR. Epidural Analgesia Saunders (W.B.) Co Ltd. 1978 (Bromage score p144)
Eponymous term review
- Pearce JM. Walter Essex Wynter, Quincke, and lumbar puncture. J Neurol Neurosurg Psychiatry. 1994 Feb;57(2):179.
- Marx GF. The first spinal anesthesia. Who deserves the laurels? Reg Anesth. 1994 Nov-Dec;19(6):429-30.
- Morgan P. Spinal anaesthesia in obstetrics. Can J Anaesth. 1995 Dec;42(12):1145-63.
- Frederiks JA, Koehler PJ. The first lumbar puncture. J Hist Neurosci. 1997 Aug;6(2):147-53.
- Marx GF. The first spinal anesthesia. Who deserves the laurels? Reg Anesth. 1994 Nov-Dec;19(6):429-30.
- Frölich MA, Caton D. Pioneers in epidural needle design. Anesth Analg. 2001 Jul;93(1):215-20.
- Goerig M, Freitag M, Standl Th. One hundred years of epidural anaesthesia—the men behind the technical development. International Congress Series, 2002; 1242: 203–212
- Ball C, Westhorpe R. Local anaesthesia–the early evolution of spinal needles. Anaesth Intensive Care. 2003 Dec;31(6):611
- Calthorpe N. The history of spinal needles: getting to the point. Anaesthesia. 2004 Dec;59(12):1231-41.
- Waurick K, Waurick R. Epiduralanästhesie – Geschichte und Technik der Epiduralanästhesie [History and Technique of Epidural Anaesthesia]. Anasthesiol Intensivmed Notfallmed Schmerzther. 2015 Jul;50(7-8):476-82
- Boulton T. Spinal anaesthesia during the 19th and 20th Centuries – cocaine and controversy. Anaesthesia News Digital April 2021
- Bowers EGM. Born on the Battlefield: Celebrating the Centennial of the Discovery of Epidural Anesthesia. Mil Med. 2021 Nov 2;186(11-12):295-296.
- López Álvarez S, Casas Reza P, Del Río Fernández S. Centenary of epidural anaesthesia. Rev Esp Anestesiol Reanim (Engl Ed). 2022 Jan;69(1):4-11
- Chinn GA, Gray AT, Larson MD. Overcoming Obstacles: The Legacy of Fidel Pagés, Founder of the Epidural, 100 Years After His Passing. Anesth Analg. 2024 Feb 1;138(2):475-479.
eponymictionary
the names behind the name

BSc MD University of Western Australia. Interested in all things critical care and completing side quests along the way
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |