
![]()
Katz-Wachtel phenomenon
Katz-Wachtel phenomenon: Tall diphasic QRS complexes (>50 mm in height) in the mid-precordial leads (leads V2, V3 or V4) typically associated with Biventricular Hypertrophy (BVH).
This is the classic ECG pattern of BVH, most commonly seen in children with congenital heart disease e.g. ventricular septal defect (VSD).
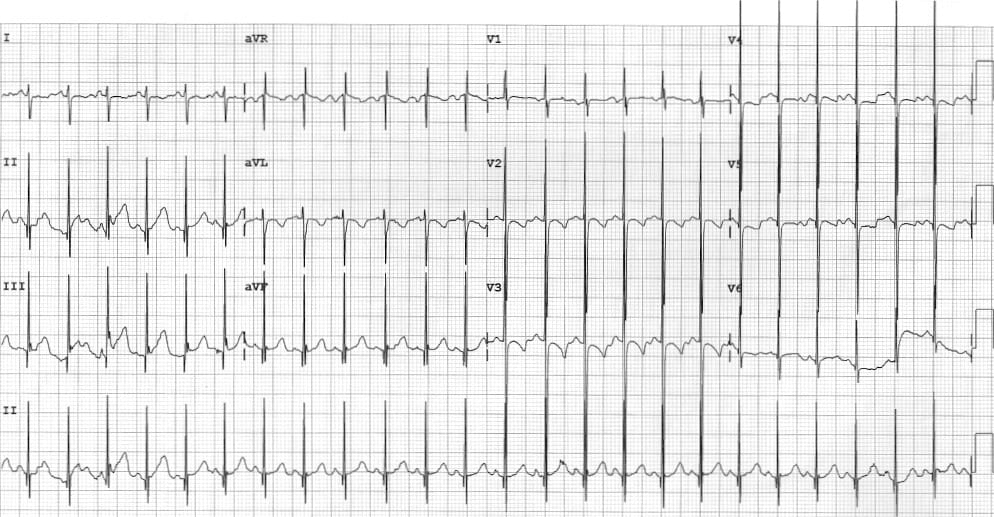
The QRS amplitude is often confusingly large overlapping other precordial leads. Repeat the ECG at half standard calibration (5mm/mV instead of 10mm/mV) allows capture of the full QRS complex without overlapping with other leads.
History of Katz-Wachtel phenomenon
1937 – Katz and Wachtel suggested that large diphasic complexes in the standard limb leads were pathognomnic of congenital heart disease. They examined the ECGs of 43 children with congenital heart disease and proposed that the QRS contour may represent combined right and left ventricular ‘strain‘
A biphasic QRS (with the size of the two phases being of the order of less than 1 to 4) was a frequent finding in congenital heart disease. The presence of such a diphasic QRS is confirmatory of this diagnosis, and, when the two phases are large and of equal extent, the finding is pathognomonic of congenital heart disease.
Katz and Wachtel, 1937
1963 – Elliott reviewed electrographic and vectorcardiographic criteris for biventricular hypertrophy. They found…
The vectorcardiograms and electrocardiograms in 10 infants with congenital malformations of the heart have been described. Each malformation demonstrated combined ventricular hypertrophy…One common denominator in each of the 10 patients was large large diphasic complexes over 50 mm in either leads V2, V3, V4 were observed in the electrocardiogram of each case of biventricular hypertrophy studied.
These tall mid-precordial QRS complexes have been called the Katz-Wachtel phenomenon and presumably reflect combined ventricular hypertrophy.
Elliott 1963
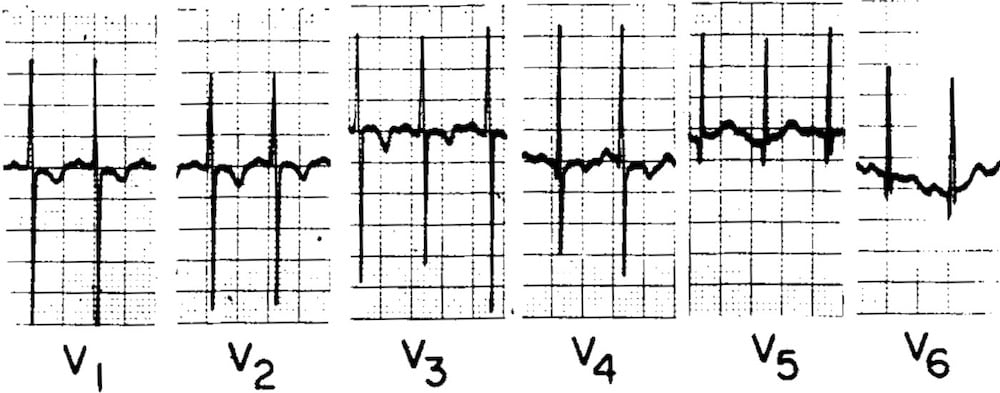
FIG. 4. Case 7. Biventricular hypertrophy in a 17 month old boy with severe anaemia and congenital deformity of the mitral valve. ECG shows biventricular hypertrophy: tall R wave in lead V1 and V2; tall RS complexes in lead Vs over 70 mm; deep S wave in lead V1; and relatively tall R waves in leads V5, and V6 preceded by a deep Q wave. Elliott 1963
Associated Persons
- Louis Nelson Katz (1897-1973)
- Hans Wachtel (1909-1977)
Alternative names
- Katz-Wachtel sign
References
- Talley JE, Fowler K. Tetralogy of Fallot (Eisenmenger type) with hypoplasia of the dextroposed aorta. The American Journal of the Medical Sciences. 1936; 191: 618-626
- Katz LN, Wachtel H. The diphasic QRS type of electrocardiogram in congenital heart disease. Am Heart J. 1937; 13: 202-206.
- Elliott LP, Taylor WP, Schiebler GL. Combined ventricular hypertrophy in infancy: Vectorcardiographic observations with special reference to the Katz-Wachtel phenomenon. Am J Cardiol. 1963;11(2):164-172
- Elliott LP, Anderson RC, Tuna N, Adams P, Neufeld HN. Complete Transposition of the Great Vessels: II. An Electrocardiographic Analysis. Circulation; 1963; 27:1118-1127.
- Patel RJ et al. Unrepaired tetralogy of fallot with right hemitruncus in an adult: a rare case. Tex Heart Inst J. 2007; 34(2): 250-251.
- Francis J. Katz Wachtel Phenomenon on ECG in VSD. 2020
- Burns E, Buttner R. Biventricular Hypertrophy. LITFL
- Cadogan M. History of the Electrocardiogram. LITFL
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
[cite]
eponymictionary
the names behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.