
![]()
Biventricular Hypertrophy
Biventricular Hypertrophy
Hypertrophy of both the left and right ventricles.
The ECG has a low sensitivity for the diagnosis of biventricular hypertrophy (BVH), as the opposing left and right ventricular forces tend to cancel each other out.
- There may be signs of both Left Ventricular Hypertrophy (LVH) and Right Ventricular Hypertrophy (RVH) on the same ECG – e.g. positive diagnostic criteria for LVH with some additional features suggestive of RVH.
- The Katz-Wachtel phenomenon – large biphasic QRS complexes in V2-5. This is the classic ECG pattern of BVH, most commonly seen in children with congenital heart disease e.g. ventricular septal defect (VSD).
In the presence of LVH – Additional signs indicating RVH include
- Right atrial enlargement.
- Right axis deviation.
- Tall biphasic QRS complexes in multiple leads.
- Deep S waves in V5-6.
In the presence of RVH – Additional signs indicating LVH include:
- Tall R waves and deep S waves in V2-5.
- QRS amplitude > 50 mm.
- Large biphasic QRS complexes (tall R waves + deep S waves) in V2-5.
ECG Examples
Example 1
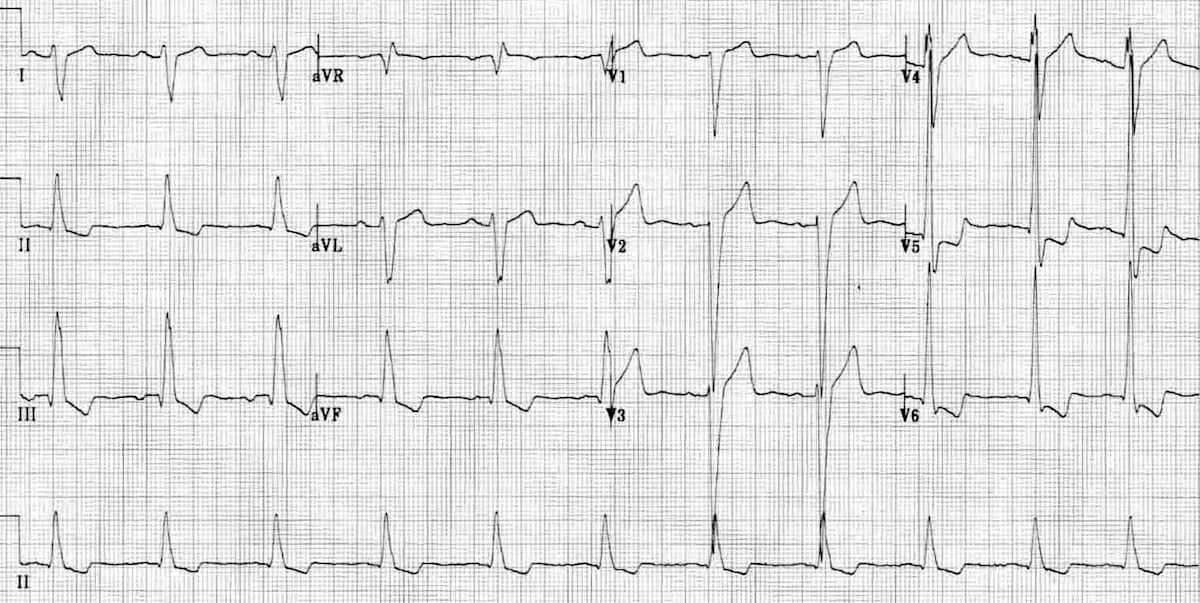
Biventricular hypertrophy:
- Large biphasic QRS complexes in V2-5.
- LVH: Voltage criteria for LVH (S V2 + R V5 = 35 mm, R aVL > 11 mm) with signs of LV strain (T-wave inversion in V4-6).
- Persistent S waves in V5-6 suggestive of associated RVH.
Example 2
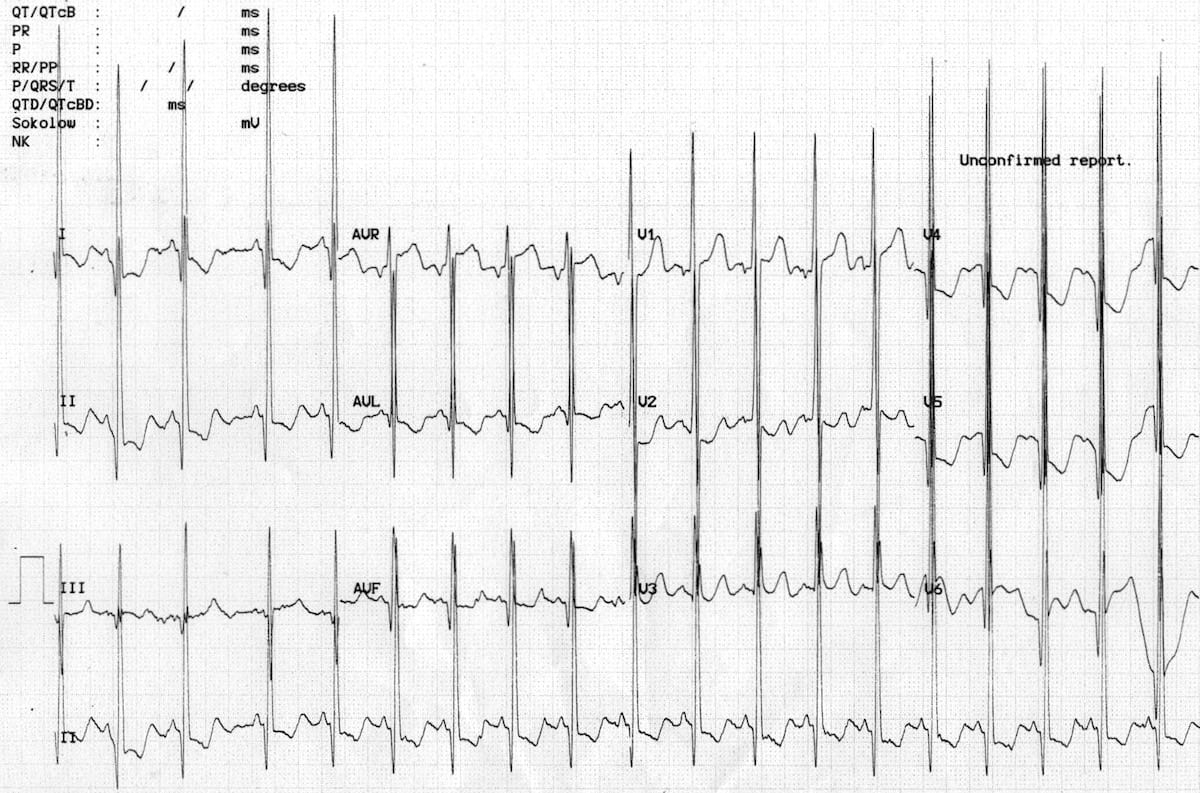
Biventricular hypertrophy
- Katz-Wachtel phenomenon — biphasic QRS complexes in the precordial leads.
- Enormous voltages — QRS amplitude > 50 mm in V2.
- Easily meets voltage criteria for LVH and there are associated features of LV strain (ST depression and T-wave inversion in V4-6).
- Signs of right atrial enlargement — peaked P waves in lead II.
Example 3
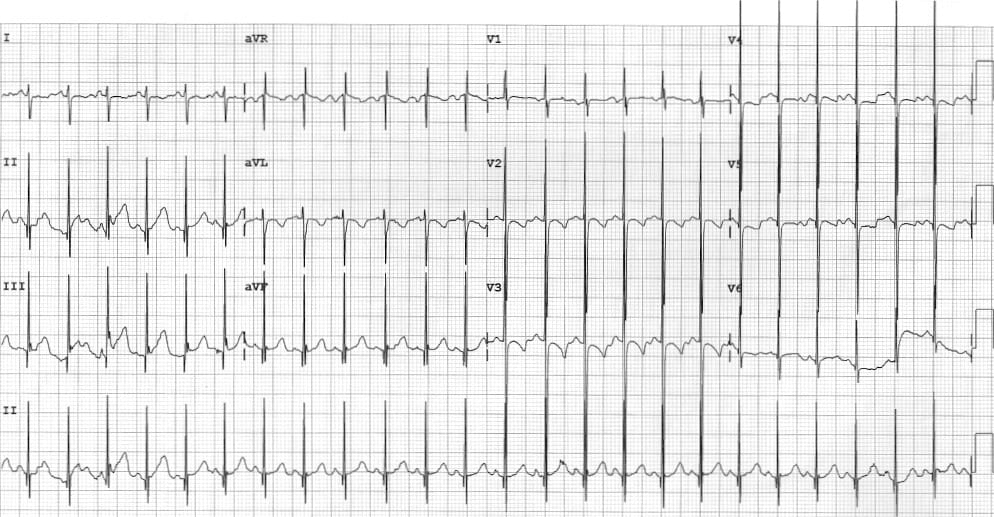
Biventricular hypertrophy in a child with VSD:
- Katz-Wachtel phenomenon – large biphasic QRS complexes in V2-5.
- Enormous QRS voltages.
- Right axis deviation and T-wave inversion in V1-3 are normal findings on the paediatric ECG.
References
- Katz LN and Wachtel H. The diphasic QRS type of electrocardiogram in congenital heart disease. Am Heart J; 1937, 13: 202-206.
- Elliott LP, Anderson RC, Tuna N, Adams P, Neufeld HN. Complete Transposition of the Great Vessels: II. An Electrocardiographic Analysis. Circulation; 1963; 27:1118-1127.
Related Topics
- Right ventricular hypertrophy
- Left ventricular hypertrophy
- Right atrial enlargement
- Left atrial enlargement
- Katz-Wachtel phenomenon
- Louis Nelson Katz (1897 – 1973)
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
ECG LIBRARY
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |
Example 1 is incorrect – there is a left arm left leg switch (not there are larger P waves high laterally then in II)
There are no persistent S waves in V5/V6
There is simply LVH with a limb lead error, it is not biventricular hyperthrophy