
![]()
R Wave Peak Time RWPT
R wave peak time is the time from onset of earliest Q wave or R wave to the peak of the R wave in the lateral leads (aVL, V5-6)
- Represents the time taken for excitation to spread from the endocardial to the epicardial surface of the left ventricle
- R-wave peak time is said to be prolonged if > 45ms
- Additionally used in Lead II in the differentiation of Ventricular Tachycardia (VT) and Supraventricular Tachycardia (SVT) with aberrancy
Causes of Prolonged RWPT

RWPT in wide QRS complex tachycardia
R-wave peak time (RWPT) may be useful in differentiating ventricular tachycardia (VT) from supraventricular tachycardia (SVT) in patients with wide QRS complex tachycardia:
- RWPT duration is measured in lead II from the onset of QRS depolarization until the first change of polarity (with both positive or negative QRS deflection)
- Studies in 2010 and 2013 demonstrated RWPT ≥ 50 ms in lead II to be a simple, reproducible, sensitive and specific for ventricular tachycardia
- However, more recent studies suggest RWPT of 50 ms may be optimal to differentiate between VT and SVT with RBBB and LAFB, but not with LBBB
Example 1
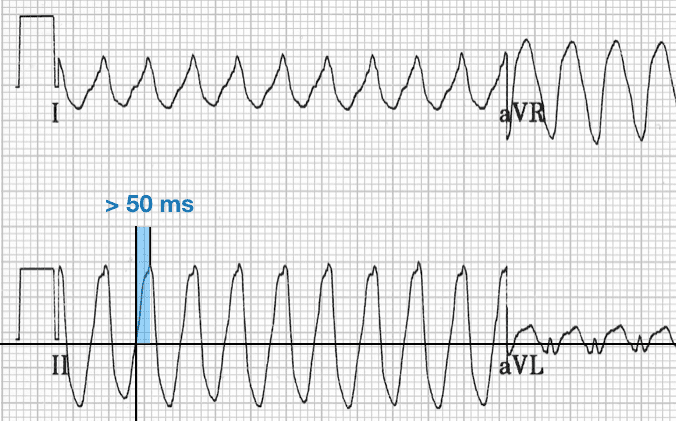
- Ventricular tachycardia
- Positive deflection wide QRS
- R-wave peak time (RWPT) >50 ms
Example 2
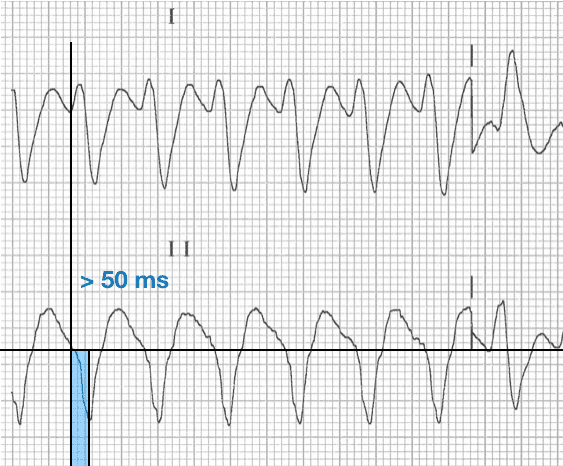
- Ventricular tachycardia
- Negative deflection wide QRS
- R-wave peak time (RWPT) >50 ms
Example 3
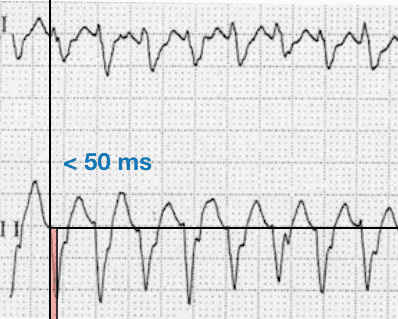
- Supraventricular tachycardia with aberrancy
- Negative deflection wide QRS
- R-wave peak time (RWPT) <50 ms
References
- Pava LF, Perafán P, Badiel M, Arango JJ, Mont L, Morillo CA, Brugada J. R-wave peak time at DII: A new criterion for differentiating between wide complex QRS tachycardias. Heart Rhythm. 2010 Jul;7(7):922-6
- Datino T, Almendral J, Avila P, González-Torrecilla E, Atienza F, Arenal A, Fernández-Avilés F. Specificity of electrocardiographic criteria for the differential diagnosis of wide QRS complex tachycardia in patients with intraventricular conduction defect. Heart Rhythm. 2013 Sep;10(9):1393-401
- Yu M et al. R-Wave Peak Time at Lead II in Adults With Ventricular Premature Beats, Bundle Branch Block and Left Anterior Fascicular Block. Am J Med Sci. 2018 Jan;355(1):44-47
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
ECG LIBRARY

MBBS DDU (Emergency) CCPU. Adult/Paediatric Emergency Medicine Advanced Trainee in Melbourne, Australia. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Co-creator of the LITFL ECG Library. Twitter: @rob_buttner
RWPT in WCT diagnosis? Neither specific [85.3% (80.6–89.3)] nor sensitive [62.0% (57.6–66.2)]. But useful when combined with other criteria in VT SCORE method. Europace (2016) 18, 578–584.
Congratulation on your web page., Marek