
![]()
R Wave Peak Time RWPT
R wave peak time is the time from onset of earliest Q wave or R wave to the peak of the R wave in the lateral leads (aVL, V5-6)
- Represents the time taken for excitation to spread from the endocardial to the epicardial surface of the left ventricle
- R-wave peak time is said to be prolonged if > 45ms
- Additionally used in Lead II in the differentiation of Ventricular Tachycardia (VT) and Supraventricular Tachycardia (SVT) with aberrancy
Causes of Prolonged RWPT

RWPT in wide QRS complex tachycardia
R-wave peak time (RWPT) may be useful in differentiating ventricular tachycardia (VT) from supraventricular tachycardia (SVT) in patients with wide QRS complex tachycardia:
- RWPT duration is measured in lead II from the onset of QRS depolarization until the first change of polarity (with both positive or negative QRS deflection)
- Studies in 2010 and 2013 demonstrated RWPT ≥ 50 ms in lead II to be a simple, reproducible, sensitive and specific for ventricular tachycardia
- However, more recent studies suggest RWPT of 50 ms may be optimal to differentiate between VT and SVT with RBBB and LAFB, but not with LBBB
Example 1
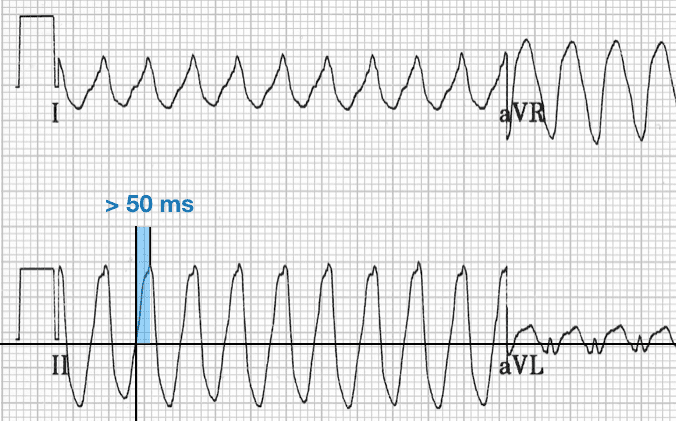
- Ventricular tachycardia
- Positive deflection wide QRS
- R-wave peak time (RWPT) >50 ms
Example 2
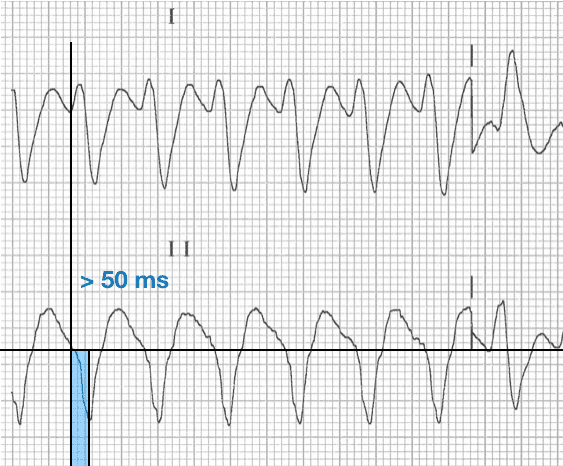
- Ventricular tachycardia
- Negative deflection wide QRS
- R-wave peak time (RWPT) >50 ms
Example 3
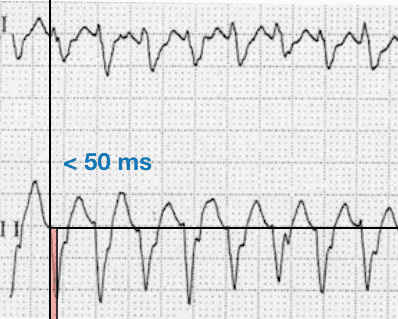
- Supraventricular tachycardia with aberrancy
- Negative deflection wide QRS
- R-wave peak time (RWPT) <50 ms
References
- Pava LF, Perafán P, Badiel M, Arango JJ, Mont L, Morillo CA, Brugada J. R-wave peak time at DII: A new criterion for differentiating between wide complex QRS tachycardias. Heart Rhythm. 2010 Jul;7(7):922-6
- Datino T, Almendral J, Avila P, González-Torrecilla E, Atienza F, Arenal A, Fernández-Avilés F. Specificity of electrocardiographic criteria for the differential diagnosis of wide QRS complex tachycardia in patients with intraventricular conduction defect. Heart Rhythm. 2013 Sep;10(9):1393-401
- Yu M et al. R-Wave Peak Time at Lead II in Adults With Ventricular Premature Beats, Bundle Branch Block and Left Anterior Fascicular Block. Am J Med Sci. 2018 Jan;355(1):44-47
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
ECG LIBRARY

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.
RWPT in WCT diagnosis? Neither specific [85.3% (80.6–89.3)] nor sensitive [62.0% (57.6–66.2)]. But useful when combined with other criteria in VT SCORE method. Europace (2016) 18, 578–584.
Congratulation on your web page., Marek