
![]()
Left Ventricular Hypertrophy (LVH)
ECG Diagnostic criteria
- There is no single universally accepted ECG definition of LVH
- ECG evidence of LVH requires a validated voltage, voltage-duration or composite criterion to be met; these criteria have high specificity but low sensitivity
- Sokolow-Lyon and Cornell criteria are among the most commonly used criteria
- Non-voltage ECG features (ST depression, T wave inversion in left-sided leads) increase diagnostic confidence but are not mandatory
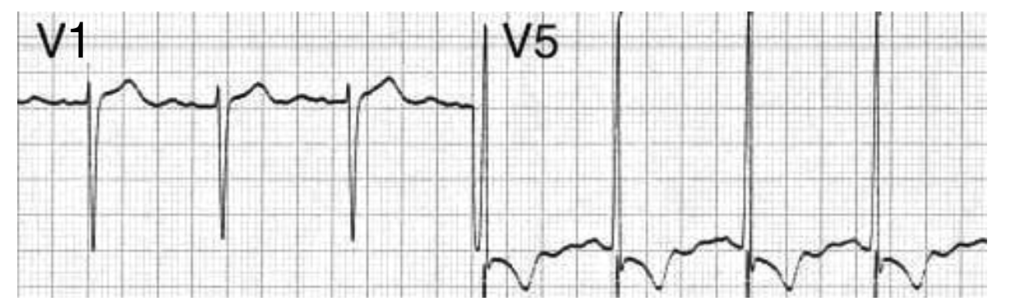
ST depression and T wave inversion in V5 are supportive features (“LV strain pattern”)
Commonly used ECG-LVH criteria [Detailed overview]
| Criterion | Diagnostic threshold |
| Sokolow–Lyon | SV1+ max(RV5,V6) ≥ 35mm |
| Cornell | RaVL+SV3 > 28mm in men, > 20mm in women |
| Peguero–Lo Presti | SD+SV4 ≥ 28mm in men, ≥ 23mm in women |
| Cornell voltage-duration product | [RaVL+SV3+8mm in women] × QRS duration > 2440 mm·ms |
| Romhilt-Estes score | ≥5 points: definite LVH; 4 points: probable LVH |
SV1 = S wave in V1, max(RV5,V6) = tallest R wave in either V5 or V6, SD = deepest S wave in any lead
Non-voltage ECG features
- Left atrial enlargement
- Left axis deviation
- ST elevation in the right precordial leads V1-3 (“discordant” to the deep S waves)
- Prominent U waves (proportional to increased QRS amplitude)

Pathophysiology
- The left ventricle hypertrophies in response to pressure overload secondary to conditions such as aortic stenosis and hypertension
- This results in increased R wave amplitude in the left-sided ECG leads (I, aVL and V4-6) and increased S wave depth in the right-sided leads (III, aVR, V1-3)
- The thickened LV wall leads to prolonged depolarisation (increased R wave peak time) and delayed repolarisation (ST and T-wave abnormalities) in the lateral leads
Causes of LVH
- Hypertension (most common)
- Aortic stenosis
- Aortic regurgitation
- Mitral regurgitation
- Coarctation of the aorta
- Hypertrophic cardiomyopathy
Handy Tips
- Voltage criteria should not be interpreted in isolation; consider repolarisation abnormalities, atrial findings, QRS duration, axis and clinical context.
- ECG changes are an insensitive means of detecting LVH (patients with clinically significant left ventricular hypertrophy seen on echocardiography may still have a relatively normal ECG)
- Anatomical confirmation requires echocardiography or cardiac MRI
ECG Examples
Example 1
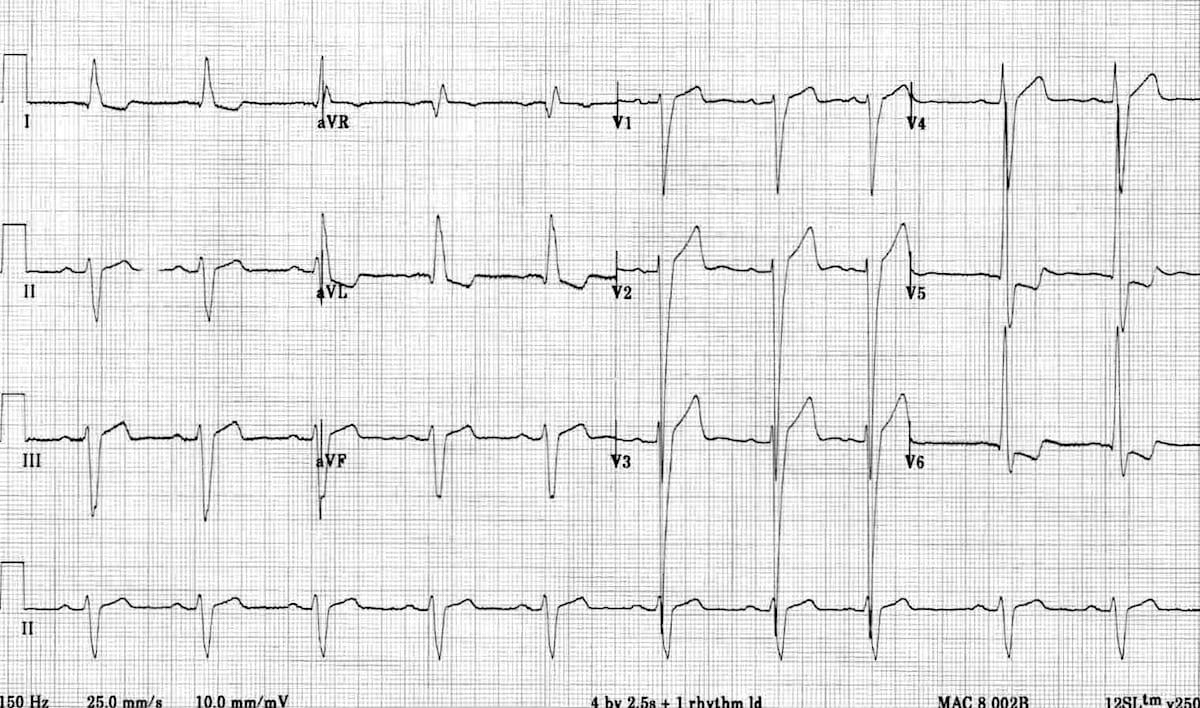
Left ventricular hypertrophy (LVH):
- Markedly increased LV voltages: huge precordial R and S waves that overlap with the adjacent leads (SV2 + RV6 >> 35 mm).
- R-wave peak time > 50 ms in V5-6 with associated QRS broadening.
- LV strain pattern with ST depression and T-wave inversions in I, aVL and V5-6.
- ST elevation in V1-3.
- Prominent U waves in V1-3.
- Left axis deviation.
Severe LVH such as this appears almost identical to left bundle branch block — the main clue to the presence of LVH is the excessively high LV voltages.
Example 2
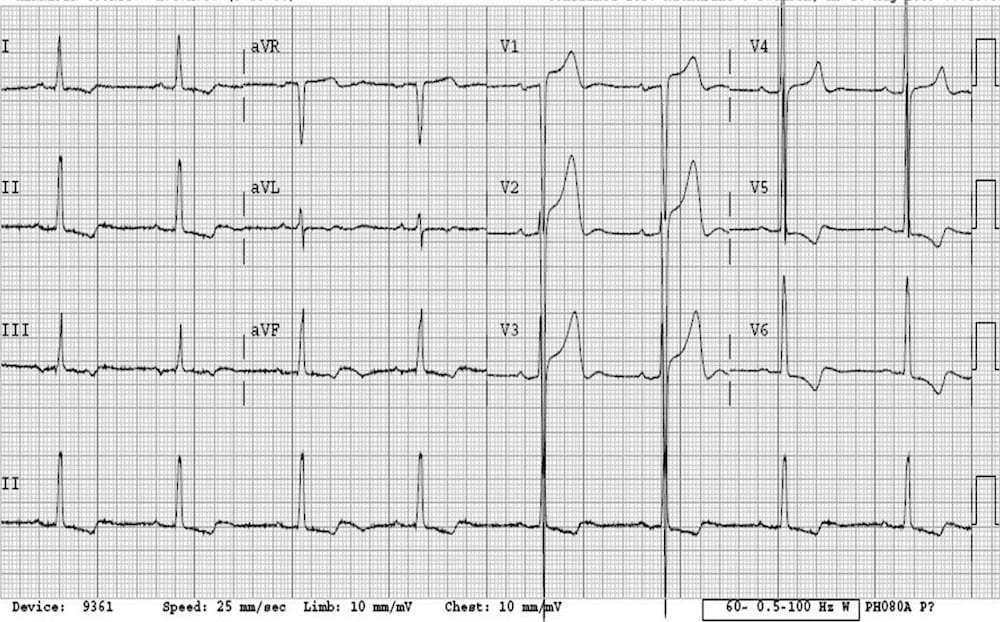
- There are massively increased QRS voltages — the S waves in V3 are so deep they are literally falling off the page!
- The ST elevation in V1-3 is simply in proportion to the very deep S waves (“appropriate discordance”).
- The LV strain pattern is seen in all leads with a positive R wave (V5-6, I, II, III, aVF).
Related Topics
- ECG criteria for left ventricular hypertrophy
- Right ventricular hypertrophy
- Left atrial enlargement
- Left bundle branch block
References
Historical references
- Sokolow M, Lyon TP. The ventricular complex in left ventricular hypertrophy as obtained by unipolar precordial and limb leads. Am Heart J. 1949 Feb;37(2):161-86 [Sokolow-Lyon criteria]
- Casale PN, Devereux RB, Alonso DR, Campo E, Kligfield P. Improved sex-specific criteria of left ventricular hypertrophy for clinical and computer interpretation of electrocardiograms: validation with autopsy findings. Circulation. 1987 Mar;75(3):565-72. [Cornell criteria]
- Molloy TJ, Okin PM, Devereux RB, Kligfield P. Electrocardiographic detection of left ventricular hypertrophy by the simple QRS voltage-duration product. J Am Coll Cardiol. 1992 Nov 1;20(5):1180-6.[Cornell Voltage-Duration Product]
- Araoye MA. Left ventricular hypertrophy by electrocardiography: A code system applicable to Negroes. Nig Postgrad Med J 1996; 3: 92-97.
Review articles
- Edhouse J, Thakur RK, Khalil JM. ABC of clinical electrocardiography. Conditions affecting the left side of the heart. BMJ. 2002 May 25;324(7348):1264-7
- Ogunlade O, Akintomide AO. Assessment of voltage criteria for left ventricular hypertrophy in adult hypertensives in south-western Nigeria. J Cardiovasc Dis Res. 2013 Mar;4(1):44-6.
- Peguero JG, Lo Presti S, Perez J, Issa O, Brenes JC, Tolentino A. Electrocardiographic Criteria for the Diagnosis of Left Ventricular Hypertrophy. J Am Coll Cardiol. 2017 Apr 4;69(13):1694-1703.
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
ECG LIBRARY
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.
does the LVH with strain pattern carry any pathologic significance? Or does it just further confirm patient has LVH.
The strain pattern just further confirms LVH. It´s presence is associated with a poor prognosis.
“…(patients with clinically significant left ventricular hypertrophy seen on echocardiography may still have a relatively normal ECG)”
–> If you see this. Think of infiltrative restrictive cardiomyopathy disease like amyloid.
Or low voltage on ECG
Just want to say that this site is the best, and you’ve helped someone start from zero with ECGs, something that scared me for a long time, much love from Egypt!
In terms of the criteria at the top of the page, there doesn’t appear to be any reference to the use of V2 when the depth of the S wave is greater than that of V1. Later examples on this page use V2 so may be worth mentioning in the criteria. This is also discussed in Garcia (2013) “The art of interpretation”.
This is a very clear and practical breakdown of LVH ECG criteria. I especially appreciated how the article highlights that voltage criteria alone are not sufficient for diagnosis and should be interpreted alongside strain patterns and clinical context. The visual examples make it much easier to connect theory with real ECG interpretation. Great resource for both learners and clinicians reviewing LVH fundamentals.