
![]()
ECG Case 065
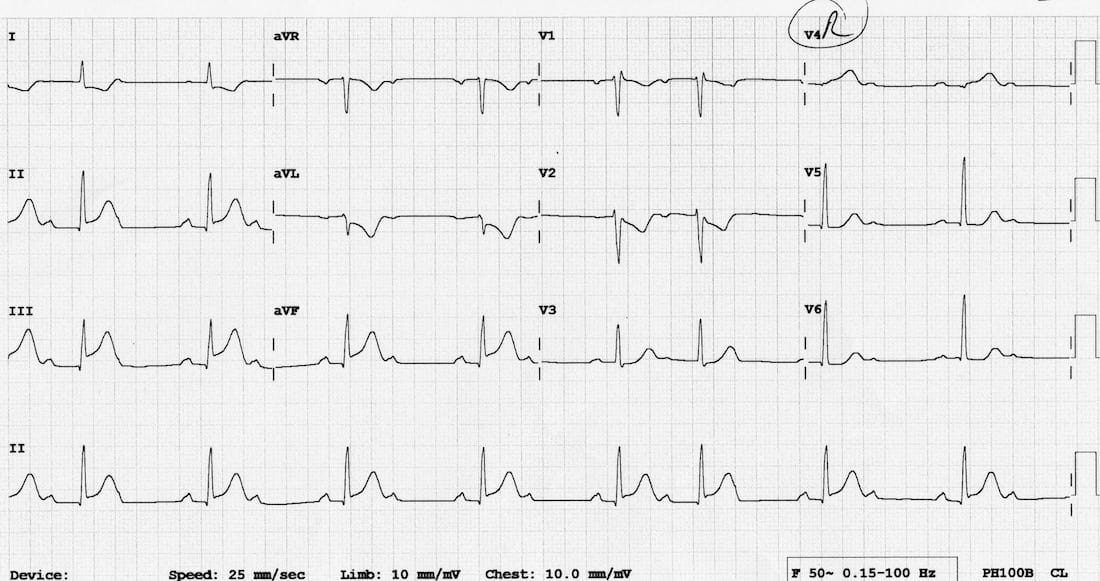
Chest pain and diaphoresis. BP 80/50. Describe and interpret his ECG
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
This is a repeat ECG of the previous patient, demonstrating:
- Inferior STEMI — STE in II, III, aVF with reciprocal change in I and aVL.
- Evidence suggesting RV infarction — STE in III > II.
- Evidence confirming RV infarction — STE and hyperacute T wave in V4R.
- Evolving second degree AV block with alternating 2:1 block and 3:2 Wenckebach cycles.
This ECG pattern is diagnostic of a right coronary artery occlusion.
Rhythm Strip Explanation

- Arrows indicate the position of P waves.
- Black arrows indicate conducted P waves.
- Red arrows indicate non-conducted P waves — some of these are concealed within the preceding T wave, causing a small bump at the back of the T wave.
- Complexes cluster together in groups with either 2:1 conduction or as 3:2 Wenckebach cycles, with prolongation of the PR interval prior to the non-conducted P wave.
- The number above each P wave denotes its position in the sequence.
CLINICAL PEARLS
Bradycardia and AV Block in Inferior STEMI
Up to 20% of patients with inferior STEMI will develop either second- or third degree heart block. Bradyarrhythmias and AV block in the context of inferior STEMI are usually transient (lasting hours to days), respond well to atropine and do not require permanent pacing.
There are three presumed mechanisms for this:
The conduction block may develop either as a step-wise progression from 1st degree heart block via Wenckebach to complete heart block (in 50% of cases) or as abrupt onset of second or third-degree heart block (in the remaining 50%).
Patients may also manifest signs of sinus node dysfunction, such as sinus bradycardia, sinus pauses, sinoatrial exit block and sinus arrest. Similarly to AV node dysfunction, this may result from increased vagal tone or ischaemia of the SA node (the SA nodal artery is supplied by the RCA in 60% of people).
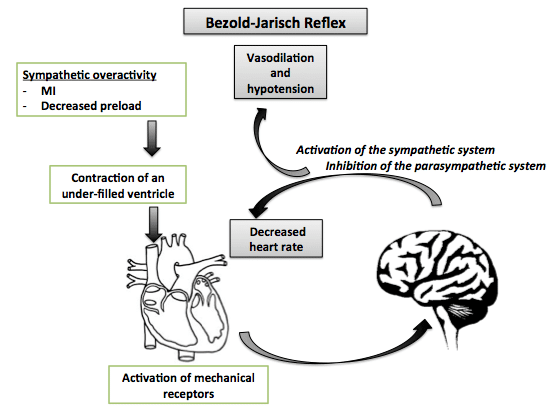
The Bezold-Jarisch reflex is an inhibitory reflex usually denoted as a cardioinhibitory reflex defined as bradycardia, vasodilation, and hypotension resulting from stimulation of cardiac receptors. In acute inferoposterior myocardial infarction:
- Cardioprotective effect: It is thought that the cardiodepressor Bezold-Jarisch reflex (BJR) acts as a protective reflex to vasodilate the coronary arteries in the setting of inferoposterior infarction associated with coronary vasospasm.
- The BJR is thought to be responsible for up to 60% of bradyarrhythmia occurring within the first 60 minutes of infarction and for the occurrence of AV nodal block in the context of acute posterior or inferior myocardial infarction.
- Reperfusion: The BJR in acute inferior myocardial infarction represents a reliable prognosticator of timely reperfusion and sustained coronary patency. It occurs in 94% of cases of successful early thrmobolysis in inferior MI; and 89% of patent right coronary artery.
- Stimulation of vagal afferents in response to sympathetic overactivity may be the underlying pathogenetic mechanism promoting a BJR response. [Clin Cardiol. 2003]
References
Further Reading
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
TOP 100 ECG Series
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |
I see this as CHB with junctional rhythm