
![]()
ECG in Chronic Obstructive Pulmonary Disease
Common ECG findings in COPD
- Rightward deviation of the P wave and QRS axis
- Low voltage QRS complexes, especially in the left precordial leads (V4-6)
- With development of cor pulmonale, right atrial enlargement (P pulmonale) and right ventricular hypertrophy
- Arrhythmias including multifocal atrial tachycardia
ECG changes occur in Chronic Obstructive Pulmonary Disease (COPD) due to:
- The presence of hyperexpanded emphysematous lungs within the chest
- The long-term effects of hypoxic pulmonary vasoconstriction upon the right side of the heart, causing pulmonary hypertension and subsequent right atrial and right ventricular hypertrophy (i.e. cor pulmonale)
Effects of Emphysema on the Heart
- Lung hyperexpansion causes external compression of the heart and lowering of the diaphragm, with consequent elongation and vertical orientation of the heart
- Due to its fixed attachments to the great vessels, the heart undergoes clockwise rotation in the transverse plane, with movement of the right ventricle anteriorly and displacement of the left ventricle posteriorly
- The presence of increased air between the heart and recording electrodes has a dampening effect, leading to reduced amplitude of the QRS complexes

Effects on the pulmonary vasculature
- Chronic hypoxaemia causes reflex vasoconstriction in the pulmonary arterioles (“hypoxic pulmonary vasoconstriction”), with consequent elevation of pulmonary arterial pressures
- Destruction of lung tissue with loss of pulmonary capillaries increases the resistance of the pulmonary vascular bed by reducing its effective surface area
- Over time, this chronic elevation of pulmonary arterial pressures results in compensatory right atrial and right ventricular hypertrophy
Typical ECG Findings in COPD
1. The most typical ECG findings in emphysema are:
- Rightward shift of the P wave axis with prominent P waves in the inferior leads and flattened or inverted P waves in leads I and aVL
- Rightward shift of the QRS axis towards +90 degrees (vertical axis) or beyond (right axis deviation)
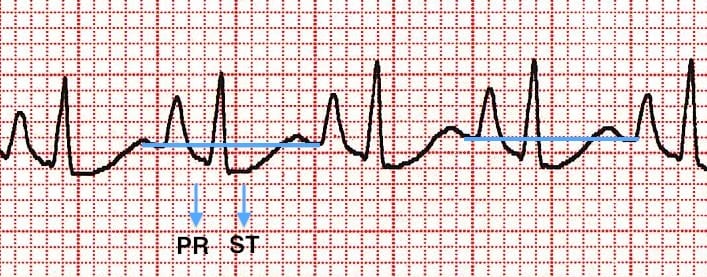
- Exaggerated atrial depolarisation causing PR and ST segments that “sag” below the TP baseline
- Low voltage QRS complexes, especially in the left precordial leads (V4-6)
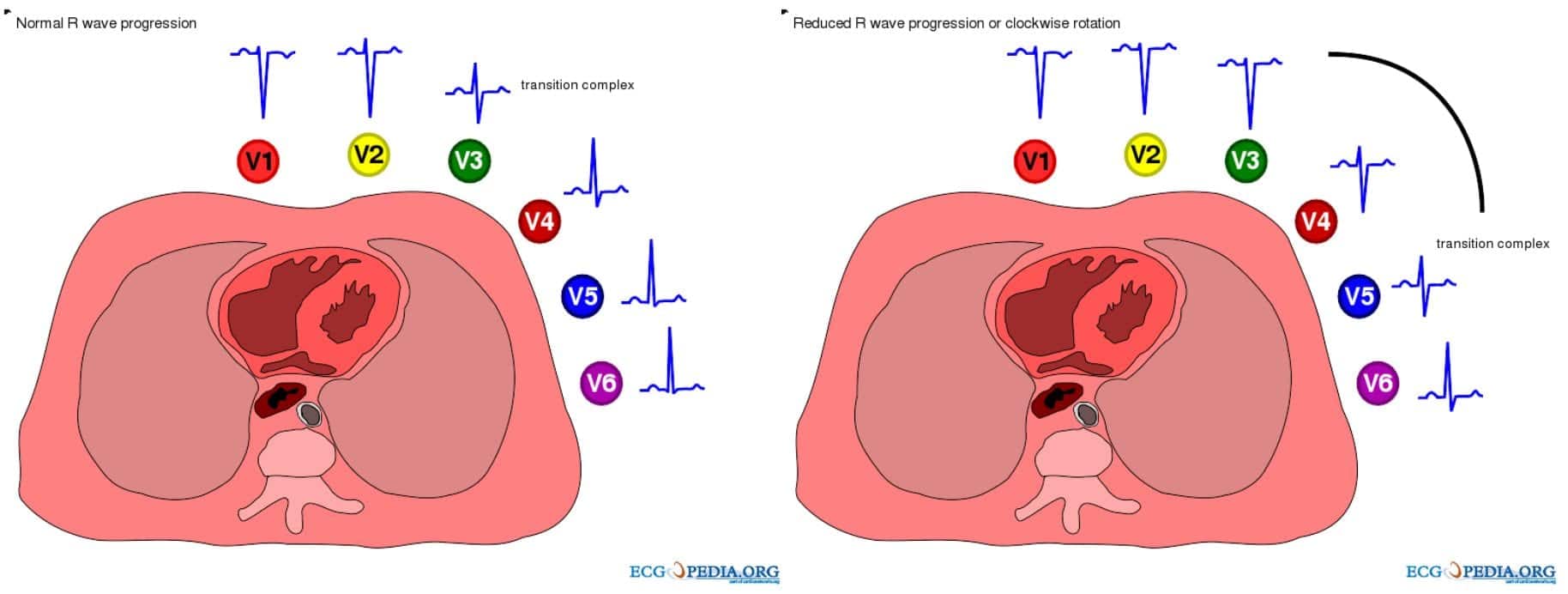
- Clockwise rotation of the heart with delayed R/S transition point in the precordial leads +/- persistent S wave in V6. There may be complete absence of R waves in leads V1-3 (the “SV1-SV2-SV3” pattern)
2. With development of cor pulmonale, the following additional changes are seen:
3. Other ECG changes that may be seen include:
- Right bundle branch block (usually due to RVH)
- Multifocal atrial tachycardia – a rapid, irregular atrial tachycardia with at least 3 distinct P wave morphologies (associated with increased mortality in patients with COPD)

Rapid, irregular, narrow-complex rhythm with at least three distinct P-wave morphologies (arrows)
ECG Examples
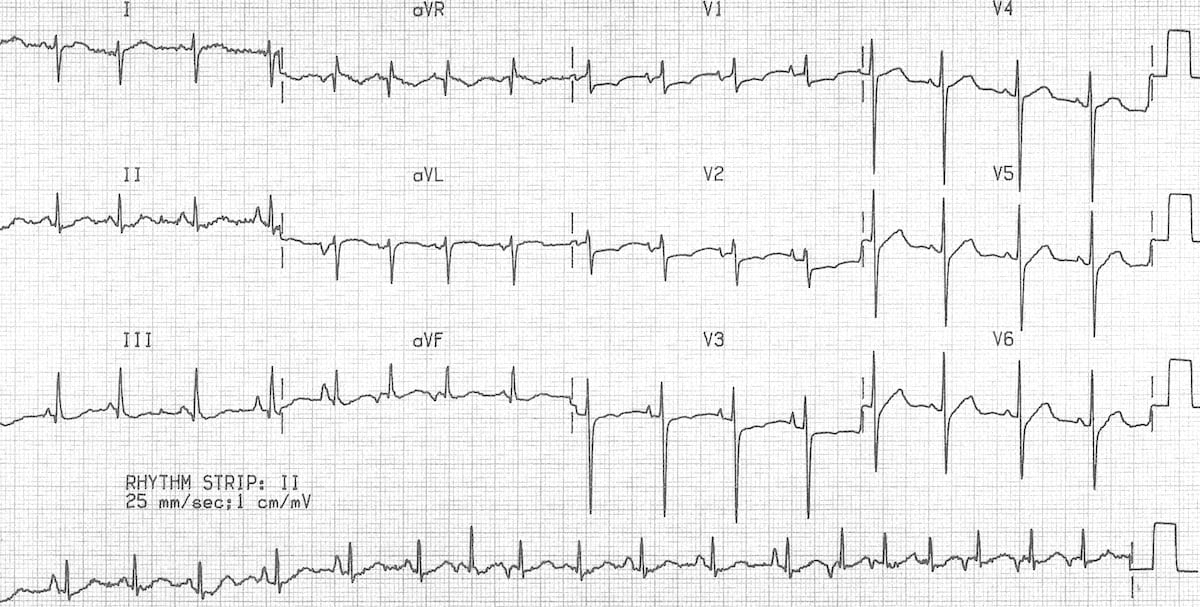
Example 1
ECG demonstrates many of the features of chronic pulmonary disease:
- Rightward QRS axis (+90 degrees)
- Peaked P waves in the inferior leads > 2.5 mm (P pulmonale) with a rightward P-wave axis (inverted in aVL)
- Clockwise rotation of the heart with a delayed R/S transition point (transitional lead = V5)
- Absent R waves in the right precordial leads (SV1-SV2-SV3 pattern)
- Low voltages in the left-sided leads (I, aVL, V5-6)
Sinus tachycardia may be due to breathlessness, hypoxia or bronchodilator therapy.
Example 2
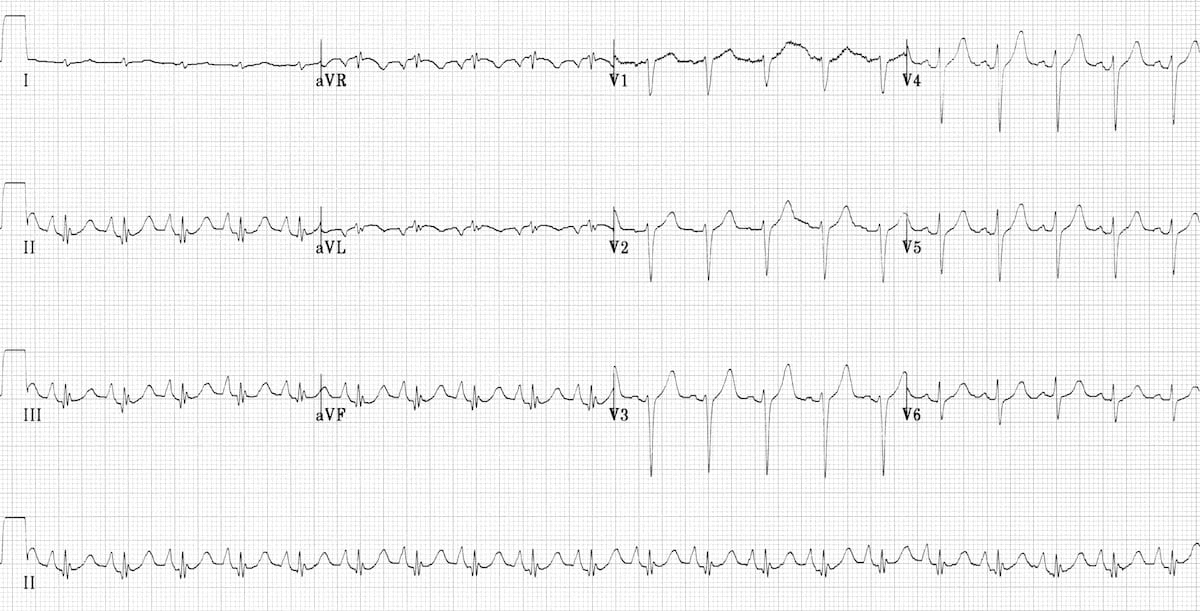
Another good example of the pulmonary disease pattern:
- Rightward axis (+ 90 degrees)
- Peaked P waves
- Low QRS voltages (most obvious in the limb leads)
- Clockwise rotation (transitional lead = V6)
- Virtually absent R waves in the right precordial leads (SV1-SV2-SV3 pattern)
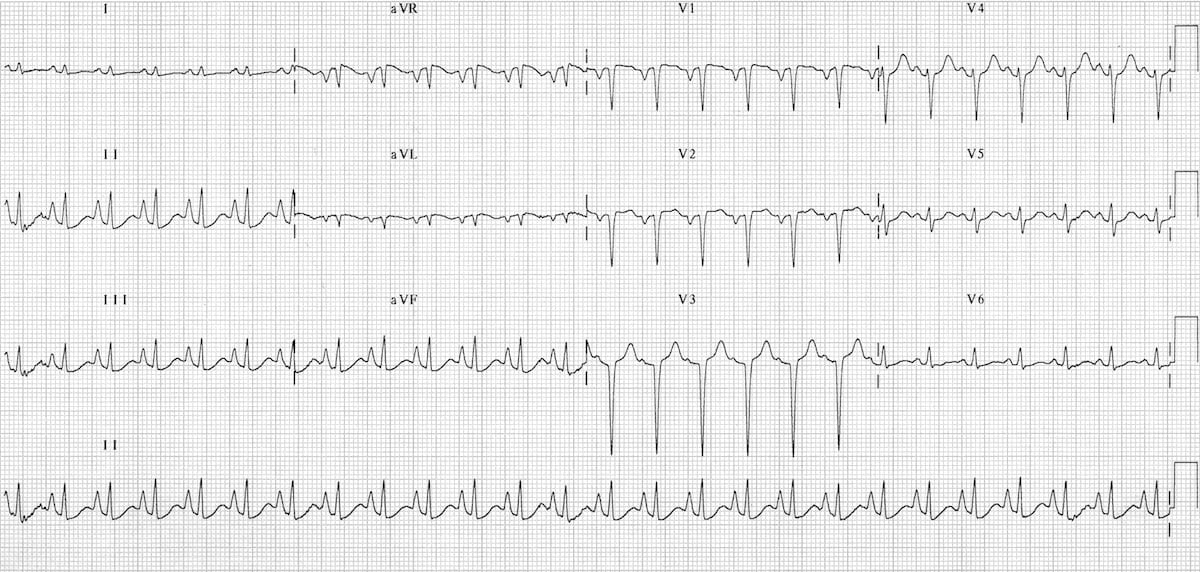
Example 3
This ECG shows multifocal atrial tachycardia with additional features of COPD:
- Rapid, irregular rhythm with multiple P-wave morphologies (best seen in the rhythm strip)
- Right axis deviation, dominant R wave in V1 and deep S wave in V6 suggest right ventricular hypertrophy due to cor pulmonale
Related Topics
- Right axis deviation
- Low voltage QRS complexes
- Right atrial enlargement (P pulmonale)
- Right ventricular hypertrophy
- Right bundle branch block
References
- Harrigan RA, Jones K. ABC of clinical electrocardiography. Conditions affecting the right side of the heart. BMJ. 2002 May 18;324(7347):1201-4
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
ECG LIBRARY
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.