
![]()
Right Ventricular Hypertrophy (RVH)
Electrocardiographic Features
Diagnostic criteria
- Right axis deviation of +110° or more.
- Dominant R wave in V1 (> 7mm tall or R/S ratio > 1).
- Dominant S wave in V5 or V6 (> 7mm deep or R/S ratio < 1).
- QRS duration < 120ms (i.e. changes not due to RBBB).
Supporting criteria
- Right atrial enlargement (P pulmonale).
- Right ventricular strain pattern = ST depression / T wave inversion in the right precordial (V1-4) and inferior (II, III, aVF) leads.
- S1 S2 S3 pattern = far right axis deviation with dominant S waves in leads I, II and III.
- Deep S waves in the lateral leads (I, aVL, V5-V6).
Other abnormalities caused by RVH
- Right bundle branch block (complete or incomplete).
ECG Pearl
There are no universally accepted criteria for diagnosing RVH in the presence of RBBB; the standard voltage criteria do not apply.
However, the presence of incomplete / complete RBBB with a tall R wave in V1, right axis deviation of +110° or more and supporting criteria (such as RV strain pattern or P pulmonale) would be considered suggestive of RVH.
Causes
- Pulmonary hypertension
- Mitral stenosis
- Pulmonary embolism
- Chronic lung disease (cor pulmonale)
- Congenital heart disease (e.g. Tetralogy of Fallot, pulmonary stenosis)
- Arrhythmogenic right ventricular cardiomyopathy
ECG Examples
Example 1
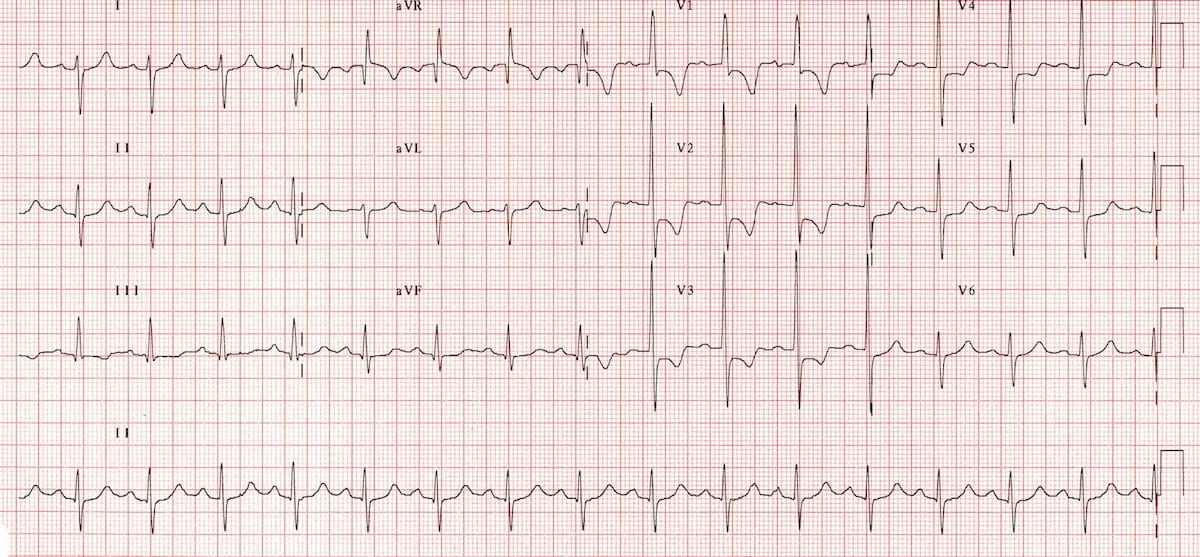
Typical appearance of RVH:
- Right axis deviation (+150 degrees).
- Dominant R wave in V1 (> 7 mm tall; R/S ratio > 1)
- Dominant S wave in V6 (> 7 mm deep; R/S ratio < 1).
- Right ventricular strain pattern with ST depression and T-wave inversion in V1-4.
Example 2
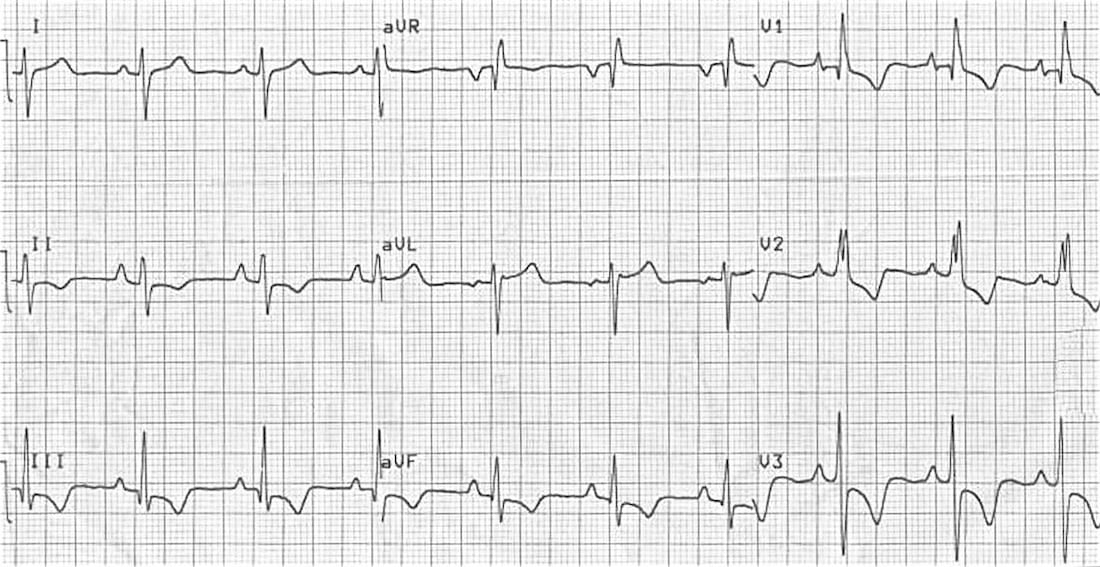
- Right axis deviation (+150 degrees)
- P pulmonale (P wave in lead II > 2.5 mm)
- Incomplete RBBB
- Right ventricular strain pattern with T-wave inversion and ST depression in the right precordial (V1-3) and inferior (II, III, aVF) leads.
This ECG was originally posted by Johnson Francis on Cardiophile.org.
Example 4

Right ventricular hypertrophy in a patient with arrhythmogenic right ventricular cardiomyopathy (ARVC):
- Right axis deviation.
- R/S ratio in V1 > 1
- Right ventricular strain pattern with T-wave inversion and ST depression in the right precordial (V1-3) and inferior (II, III, aVF) leads.
This ECG was originally posted by Jayachandran Thejus on the website HeartPearls.com.
Related Topics
- Right ventricular strain.
- The ECG in pulmonary embolism.
- The ECG in chronic lung disease.
- Left ventricular hypertrophy.
References
- Harrigan RA, Jones K. ABC of clinical electrocardiography. Conditions affecting the right side of the heart. BMJ. 2002 May 18;324(7347):1201-4. Review. PMID: 12016190
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
ECG LIBRARY
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.
in your last example, please notice diffuse epsilon waves in arvc