
![]()
Marathon-related ECG Exasperation
aka ECG Exigency 005
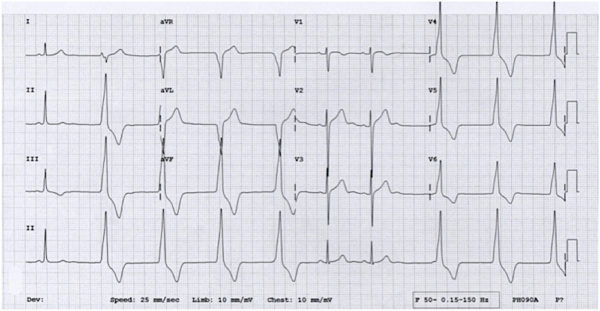
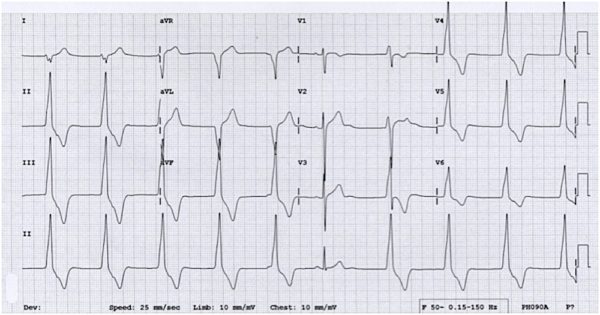
The following two ECGs were taken from a 36-year old marathon runner presenting to the ED with acute gastroenteritis.
He was completely asymptomatic at the time the ECGs were taken, with normal blood pressure and no chest pain, palpitations or dizziness. Electrolytes were normal.
Questions
Q1. What are the ECG findings?
Answer and Interpretation
ECGs findings include:
- Accelerated idioventricular rhythm (AIVR) at around 60 bpm
- Multiple sinus capture beats
- Isorhythmic AV dissociation: Sinus P waves are buried in the QRS complexes and T waves at a similar rate to the ventricular rhythm – best seen in the rhythm strip in ECG # 2
- Sinus arrhythmia, with variation in the PP interval of up to 0.2 s
Summary
- Competing sinus and idioventricular pacemakers are present.
- There is underlying sinus arrhythmia, with sinus capture occurring when the sinus rate exceeds the idioventricular rate.
Definitions
Accelerated idioventricular rhythm:
- An ectopic ventricular rhythm consisting of three or more ventricular complexes occurring at a rate of 50-110 bpm.
- The rate differentiates AIVR from ventricular escape rhythms (rate < 50 bpm) and VT (> 110bpm).
Isorhythmic AV dissociation:
- AV dissociation with sinus and ventricular complexes occurring at similar rates, unlike 3rddegree heart block where the atrial rate is usually faster than the ventricular rate.
- Isorhythmic AV dissociation is usually due to functional block at the AV node from retrogradely conducted ventricular impulses (“interference-dissociation”), which leaves the AV node refractory to the anterograde sinus impulses.
Sinus arrhythmia:
- Sinus rhythm in which the PP interval varies by 0.16 s or more.
Q2. What is the mechanism of this arrhythmia?
Answer and Interpretation
The likely mechanism of the AIVR in this patient is enhanced automaticity of an ectopic pacemaker in the ventricles coupled with sinus bradycardia and sinus arrhythmia due to athletic training.
There are pacemaker cells at various sites throughout the conducting system, with each site capable of independently sustaining the heart rhythm. The rate of spontaneous depolarisation of pacemaker cells decreases down the conducting system:
- SA node (60-100 bpm)
- Atria (< 60 bpm)
- AV node (40-60 bpm)
- Ventricles (20-40 bpm)
Under normal conditions, subsidiary pacemakers are suppressed by the more rapid impulses from the sinus node. AIVR occurs when the rate of an ectopic ventricular pacemaker exceeds that of the sinus node.
- Athletic training leads to changes in the autonomic nervous system, with increased resting vagal tone and decreased sympathetic tone.
- This hypervagotonic state causes suppression of impulse generation by the SA node and propagation by the AV node.
- As a result, athletic individuals will commonly exhibit sinus bradycardia and low-grade AV blocks (e.g. 1st degree heart block, Mobitz I).
Q3. What are the other causes of this arrhythmia?
Answer and Interpretation
AIVR is most commonly seen during the reperfusion phase of an acute myocardial infarction. It is also seen with:
- Drug toxicity, especially digoxin, cocaine and volatile anaesthetics such as desflurane
- Electrolyte abnormalities
- Cardiomyopathy
- Congenital heart disease
- Myocarditis
- Following return of spontaneous circulation in the post-cardiac-arrest period
Q4. What other ECG abnormalities are common in athletes?
Answer and Interpretation
The following abnormalities may be present, due to autonomic conditioning (enhanced vagal tone, decreased sympathetic tone) and ventricular hypertrophy:
- Sinus arrhythmia
- Sinus bradycardia
- Junctional or ventricular escape rhythms
- 1st degree heart block
- Wenckebach phenomenon
- Left ventricular hypertrophy
- Axis deviation
- Incomplete RBBB
Q5. How should this rhythm be managed?
Answer and Interpretation
Management
- AIVR is a benign rhythm in most settings and does not usually require treatment.
- Administration of anti-arrhythmics may cause precipitous haemodynamic deterioration and should be avoided.
- Treat the underlying cause:
- correct electrolytes
- restore myocardial perfusion
- give Digibind in the case of digoxin toxicity.
- Patients with low-cardiac-output states (e.g. dilated cardiomyopathy) may benefit from restoration of AV synchrony to restore atrial ’kick’ – in this case atropine may be used to increase sinus rate and AV conduction
References
- Riera ARP, Barros RB, de Sousa FD, Baranchuk A. Accelerated Idioventricular Rhythm: History and Chronology of the Main Discoveries. Indian Pacing and Electrophysiology Journal;2010; 10(1):40-48 [PMC 2803604]
- Hampton, JR. The ECG In Practice, 6e
- Mattu A, Brady W. ECG’s for the Emergency Physician 1
- Mattu A, Brady W. ECGs for the Emergency Physician 2
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric, 6e
- Wagner, GS. Marriott’s Practical Electrocardiography 12e
Further Reading
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF

CLINICAL CASES
ECG EXIGENCY
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |
Thank you very much Sir. I am so so grateful to you sir for getting a lot of knowledge and informations in ECG and Cardiology.
Thanks for making really complicated things comprehensible. Your articles are excellent and a really good resource.
Agree!
Thank you so much for such important information. Your page has helped me a lot!