
![]()
Junctional Escape Rhythm
ECG features of Junctional Escape Rhythm
- Junctional rhythm with a rate of 40-60 bpm
- QRS complexes are typically narrow (< 120 ms)
- No relationship between the QRS complexes and any preceding atrial activity (e.g. P-waves, flutter waves, fibrillatory waves)
Mechanism
Pacemaker cells are found at various sites throughout the conducting system, with each site capable of independently sustaining the heart rhythm. The rate of spontaneous depolarisation of pacemaker cells decreases down the conducting system:
- SA node (60-100 bpm)
- Atria (< 60 bpm)
- AV node (40-60 bpm)
- Ventricles (20-40 bpm)
Under normal conditions, subsidiary pacemakers are suppressed by the more rapid impulses from above (i.e. sinus rhythm). Junctional and ventricular escape rhythms arise when the rate of supraventricular impulses arriving at the AV node or ventricle is less than the intrinsic rate of the ectopic pacemaker.
Causes
Conditions leading to the emergence of a junctional or ventricular escape rhythm include:
- Severe sinus bradycardia
- Sinus arrest
- Sino-atrial exit block
- High-grade second degree AV block
- Third degree AV block
- Hyperkalaemia
- Drugs: beta-blocker, calcium-channel blocker or digoxin poisoning
ECG Examples
Example 1
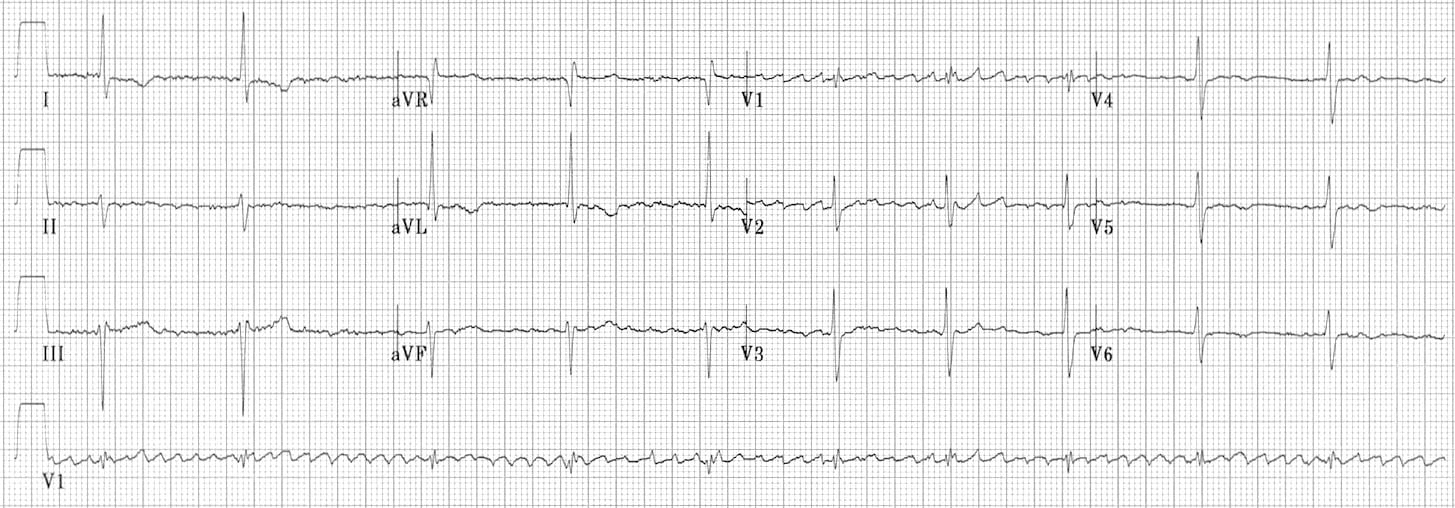
Atrial fibrillation with 3rd degree AV block and a junctional escape rhythm (“regularised AF”)
- Coarse atrial fibrillation (irregular baseline with atrial complexes at rate > 400 bpm)
- Regular narrow complex rhythm at 60 bpm
- The combination of atrial fibrillation with a regular rhythm (“regularised AF”) indicates that none of the atrial impulses are conducted to the ventricles, i.e. complete heart block is present
- The narrow complex rhythm is therefore a junctional escape rhythm
- Regularised AF is characteristically seen as a consequence of digoxin toxicity
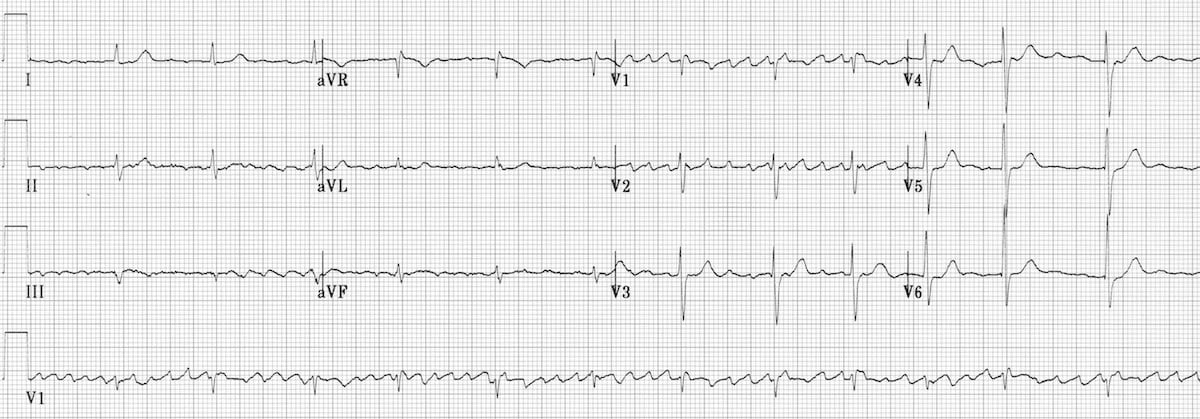
Example 2
Terminology of junctional rhythms
- Junctional bradycardia = junctional rhythm at a rate of < 40 bpm
- Junctional escape rhythm = junctional rhythm at a rate of 40-60 bpm
- Accelerated junctional rhythm = junctional rhythm at 60-100 bpm
- Junctional tachycardia = junctional rhythm at > 100 bpm
Related Topics
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
ECG LIBRARY
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.
I dont agree with the first example as atrial fibrillation
Its more like atrial flutter with variable block
I’m confident it’s AF. I see the point, but you’d expect each flutter wave in atrial flutter to circle around the same macrore-entry circuit (e.g. tricuspid annulus). Therefore, flutter waves with (almost) always have identical morphology. It’s different here, so has to be coarse AF.
That is AF, those are coarse fib waves not flutter waves
No fluther waves in II, III, Avf. That is more likely coarse a fib.
Is the 2nd example, Atrial Flutter with Junctional Escape Rhythm? (since there there is 3 consecutive junctional beats in aVR)