
![]()
Right Ventricular Strain
Right ventricular strain is a repolarisation abnormality due to right ventricular hypertrophy (RVH) or dilatation.
ECG Features
ST depression and T wave inversion in leads corresponding to the right ventricle:
- Right precordial leads V1-3 +/- V4
- Inferior leads II, III, aVF, often most pronounced in lead III as this is the most rightward facing lead
Associated features often include those seen in RVH:
- Right axis deviation
- Dominant R wave in V1
- Dominant S wave in V5 or V6
Compare this to the left ventricular strain pattern, where ST/T-wave changes are present in the left ventricular leads (I, aVL, V5-6).
Causes
Associated with increased pulmonary artery pressures in the setting of acute or chronic right ventricular hypertrophy or dilatation:
- Pulmonary hypertension
- Mitral stenosis
- Pulmonary embolism
- Chronic lung disease (cor pulmonale)
- Congenital heart disease (e.g. Tetralogy of Fallot, pulmonary stenosis)
- Arrhythmogenic right ventricular dysplasia (ARVD)
ECG Examples
Example 1
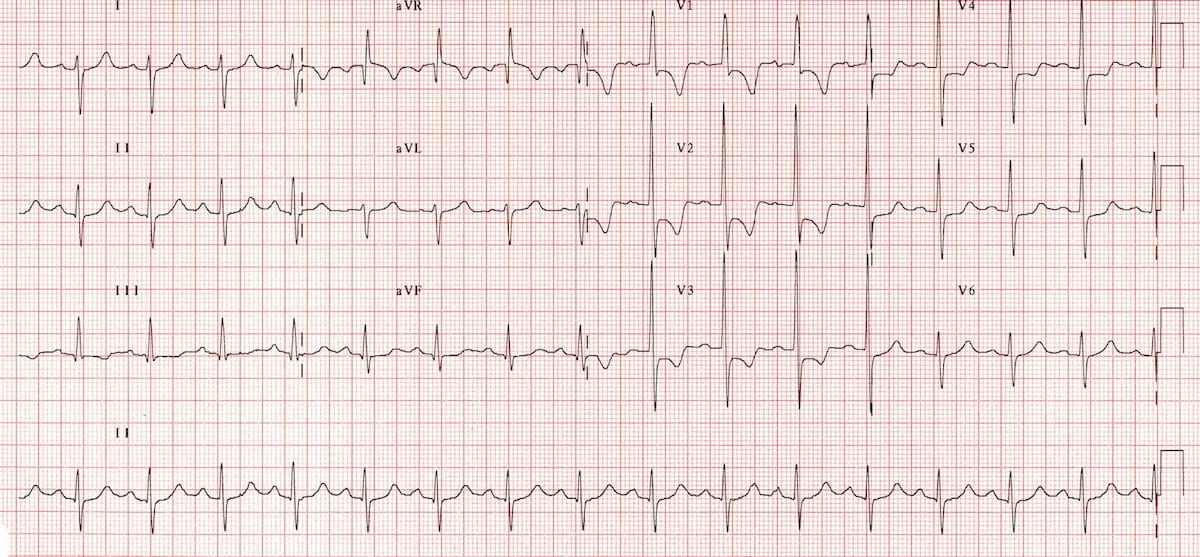
Right ventricular strain pattern due to RVH:
- ST depression and T-wave inversion in V1-4 and lead III
- Other features of RVH are present, including right axis deviation, and a dominant R wave in V1
Example 2
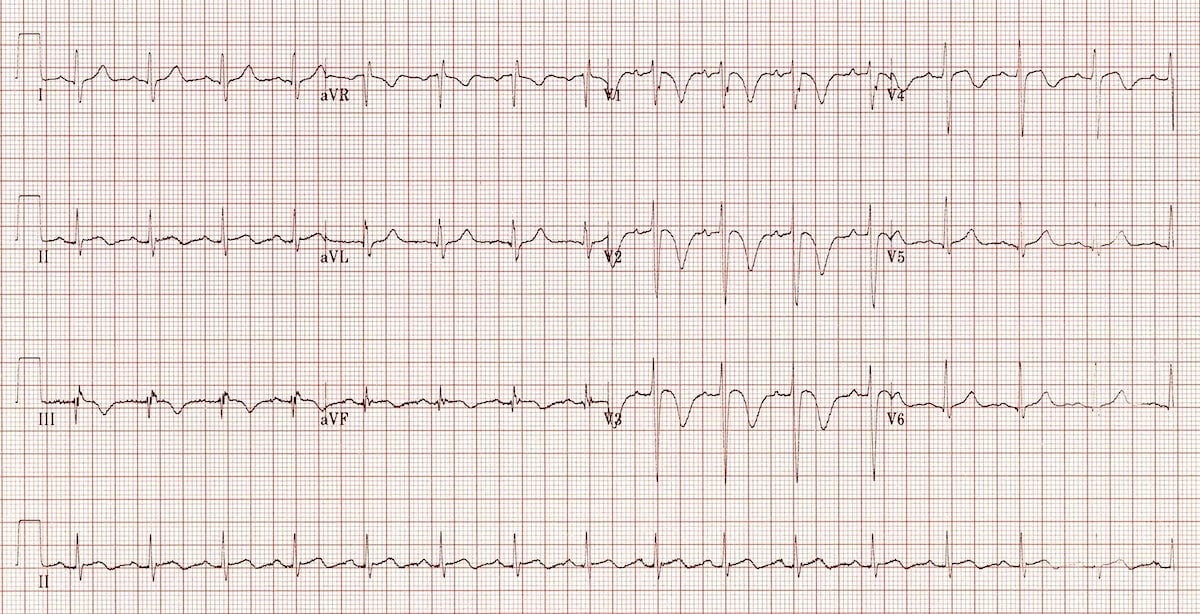
Right ventricular strain pattern due to acute right ventricular dilatation:
- T-wave inversions are seen in the right precordial (V1-4) and inferior leads (III, aVF)
- This patient had a massive pulmonary embolism
Related Topics
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
ECG LIBRARY
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |
Is there be a good method to differentiate these TWI from strain or Wellens type T waves? In example 2 they seem to look particularly similar to either.
Hi Will,
Differentiation between the two can sometimes be difficult on ECG alone. In example 2, T wave inversion extending to inferior leads is more suggestive of RV strain and specifically PE. In Wellens, T wave inversion is usually isolated to precordial leads.
Most of the time, there will also be associated features of RVH (RAD, dominant R wave in V1) or other underlying pathology such as PE (sinus tachycardia, right axis deviation, RBBB morphology). In addition, clinical context will assist.
I hope this helps.
Rob