
![]()
VT versus SVT: It’s as easy as ABCDE
VT or not VT…that is the question
Most of us know this question all to well. We are also probably familiar with the long list of ECG features “suggestive” of ventricular tachycardia (VT). Unfortunately, this list is not always intuitive, and can be difficult to recall and apply under pressure on the floor.
How can we simplify things?
I’ve spent the last few days coming up with a more easily applicable approach to this common dilemma.
A quick disclaimer before we start…
- Before we look at the trace, we should know that 70% of regular wide complex tachycardia (WCT) is VT. History of MI, structural heart disease, and/or old age makes VT even more likely
- No single ECG feature is “diagnostic” of VT
- However, the presence of any of the following five ECG features is highly specific for VT (90-100%)
Introducing the ABCDE approach — FIVE quick, simple questions to ask yourself…
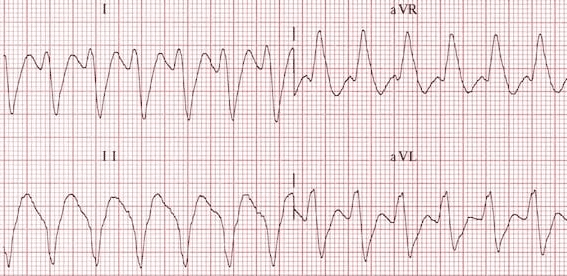
#1: A is for Axis
Is there a Northwest axis?
Presence of a Northwest axis (-90 to -180 degrees) is highly specific for VT (90%).
Look for a dominant R wave in aVR for quick reference. Always consider metabolic disturbance (K, Na channel blockade, acidosis).
#2: B is for Broad complexes
Use a cut-off of > 200ms, which has a specificity of 85-90% for VT. Below this, there is too much overlap between VT and SVT with aberrancy.
Note that variants such as Right Ventricular Outflow Tract (RVOT) VT may demonstrate shorter QRS durations – as such, a narrower QRS does not exclude VT.
#3: C is for Concordance
If you gave me just one question, this would be it – does the QRS complex resemble any form of aberration?
- If so, SVT is probable
- If not, VT or antidromic AVRT is probable
Precordial concordance (a lack of RS complex in V1-6) is 97% specific for VT.
Positive concordance (left) refers to entirely positive complexes in lead V1-6, with no rS complexes seen. Vice versa, negative concordance (right) is entirely negative (QS) complexes in V1-6.
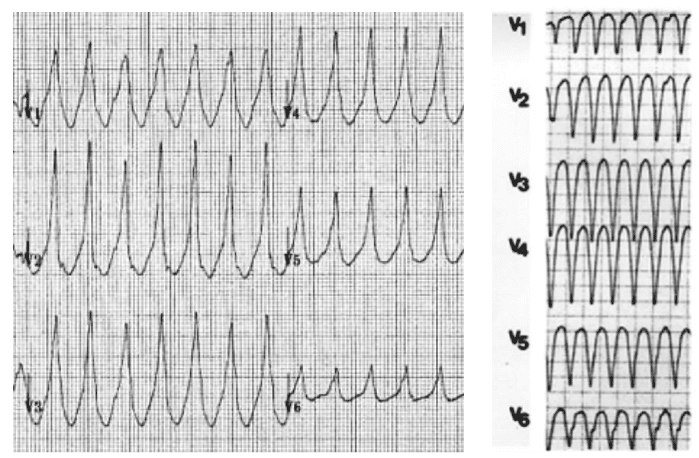
Negative concordance (right): Entirely negative (QS) complexes in V1-6
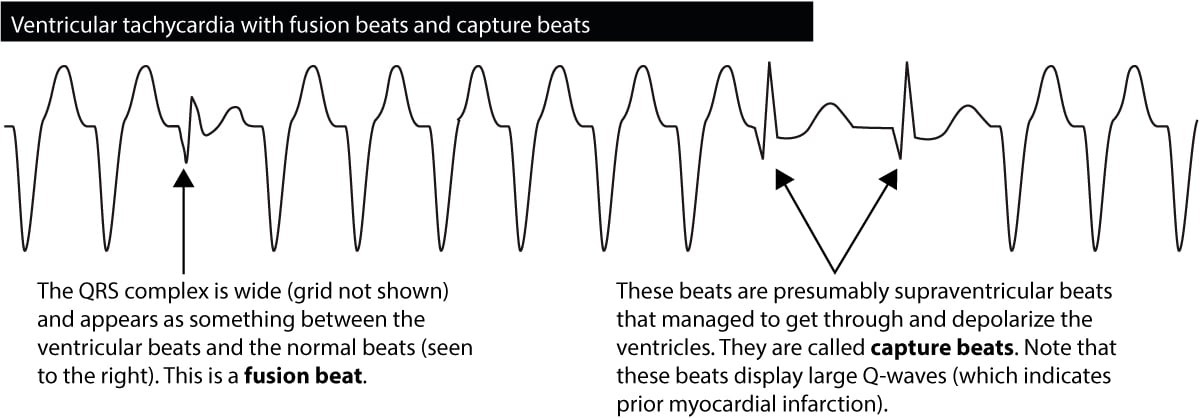
#4: D is for Dissociation
Is there AV dissociation?
Any evidence of AV dissociation is highly specific for VT:
- P and QRS complexes at different rates
- Capture beats: where the SA node transiently “captures” the ventricles, producing an isolated normal QRS complex
- Fusion beats: Occur when a sinus and ventricular beat coincide to produce a hybrid complex (see Dressler beat)
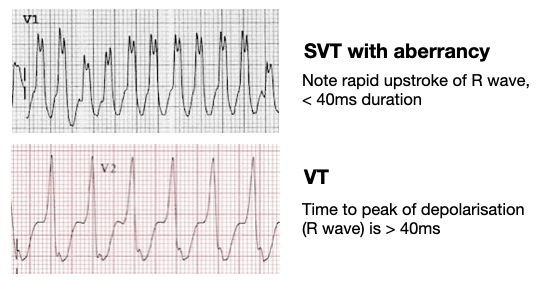
#5: E is for Early part of QRS
Is the early part of the QRS fast or slow?
SVT with aberrancy and VT differ in the way that they engage the His-Purkinje network:
- VT propagates from ventricular muscle, with initial slow myocyte-to-myocyte conduction time. This causes a delayed/slurred initial QRS component
- SVT with aberrancy displays initial sharp QRS deflections that arise from the preserved bundle branch
The “VT score”
Although the presence of any of the above points towards VT, I’m a numbers person. If time permits, I like to know the exact probability I am dealing with.
For this, the VT score is perfect. It utilises criteria with a high specificity to give us a percentage likelihood this is VT.
Any score of 3 or over is 99.6-100% specific for VT.
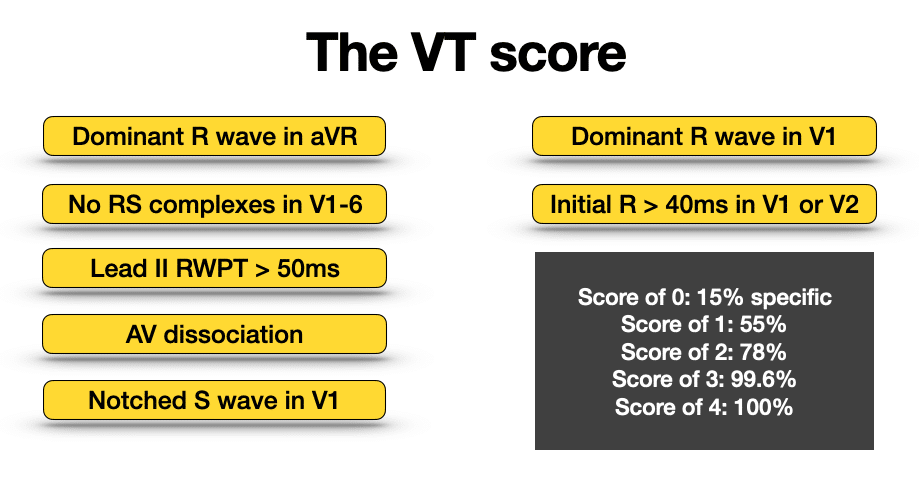
As you can see, it is made up largely of the ABCDE approach we discussed above.
A notched S wave in V1 (otherwise known as Josephson sign) is another highly specific sign of VT (97-100%). It is a fragmentation of the nadir of the S wave, probably caused by fibrosis due to previous infarctions.
You could probably make it the ABCDEF approach, with F for fragmentation of the S wave in V1.
You can’t win every time…
So, with these tools we can now be sure every time right?
Unfortunately not. Even with a structured approach, some rhythms remain in doubt.
- In unstable patients the decision is easy – they need electricity
- In stable patients with regular wide complex tachycardia, consider doubling the paper speed, utilising the Lewis Lead, or trialling adenosine
Further useful reading
LITFL ECG Library
- VT versus SVT
- Monomorphic VT
- Supraventricular tachycardia (SVT)
- Right ventricular outflow tract (RVOT) VT
The VT Score
- Jastrzebski et al. The ventricular tachycardia score: a novel approach to electrocardiographic diagnosis of ventricular tachycardia. EP Europace, Volume 18, Issue 4, April 2016, Pages 578–584
Safety of adenosine in regular wide complex tachycardia
- Marill et al. Adenosine for wide-complex tachycardia: efficacy and safety. Crit Care Med. 2009 Sep;37(9):2512-8
- Harris P, Lysitsas D. Ventricular arrhythmias and sudden cardiac death. BJA Education. 2016; 16(7): 221-229
Further reading
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course – Become an ECG expert. Medmastery
- Wiesbauer F, Kühn P. ECG Blue Belt online course: Learn to diagnose any rhythm problem. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
ECG LIBRARY

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.
Thanks for sharing, Rob! In addition, I’ve always thought “ABC” would have been a more appropriate song for ACLS. 94bpm and a casual reminder of the ABC’s.
A really succinct tool and easy to use. Many thanks
BRILLIANT- many thanks, Rob! 🙏
Great job Rob!
When talking to students, we always cite the great Amal Mattu’s mantra: WCT is VT until proven otherwise —> go to electricity.
Roberto