
![]()
Abdominal CT: closed loop
Identifying closed loop small bowel obstruction
A closed loop small bowel obstruction is defined by two points of obstruction which effectively isolates a loop (i.e., segment) of small bowel from the rest of the gastrointestinal tract.
Closed loop small bowel obstructions often require urgent surgery, but they can be difficult to confidently diagnose. It is essential to catch this diagnosis, as the patient is at risk for intestinal ischemia, perforation, and a complicated postoperative experience without prompt surgical intervention.
Closed loop obstructions are most commonly associated with
- Adhesions
- Hernias
- Volvulus

Adhesions
Closed loop small bowel obstruction is most commonly caused by adhesions (i.e., scar tissue) tethering the small bowel. The two points of obstruction are typically next to each other as they share a common cause.
Example 1
In the abdominal CT we see a segment of small bowel trapped by adhesion at two points. You can identify these points of obstruction by tracing the bowel in and out of the closed loop, noting that they are next to each other and that they make sharp angles.
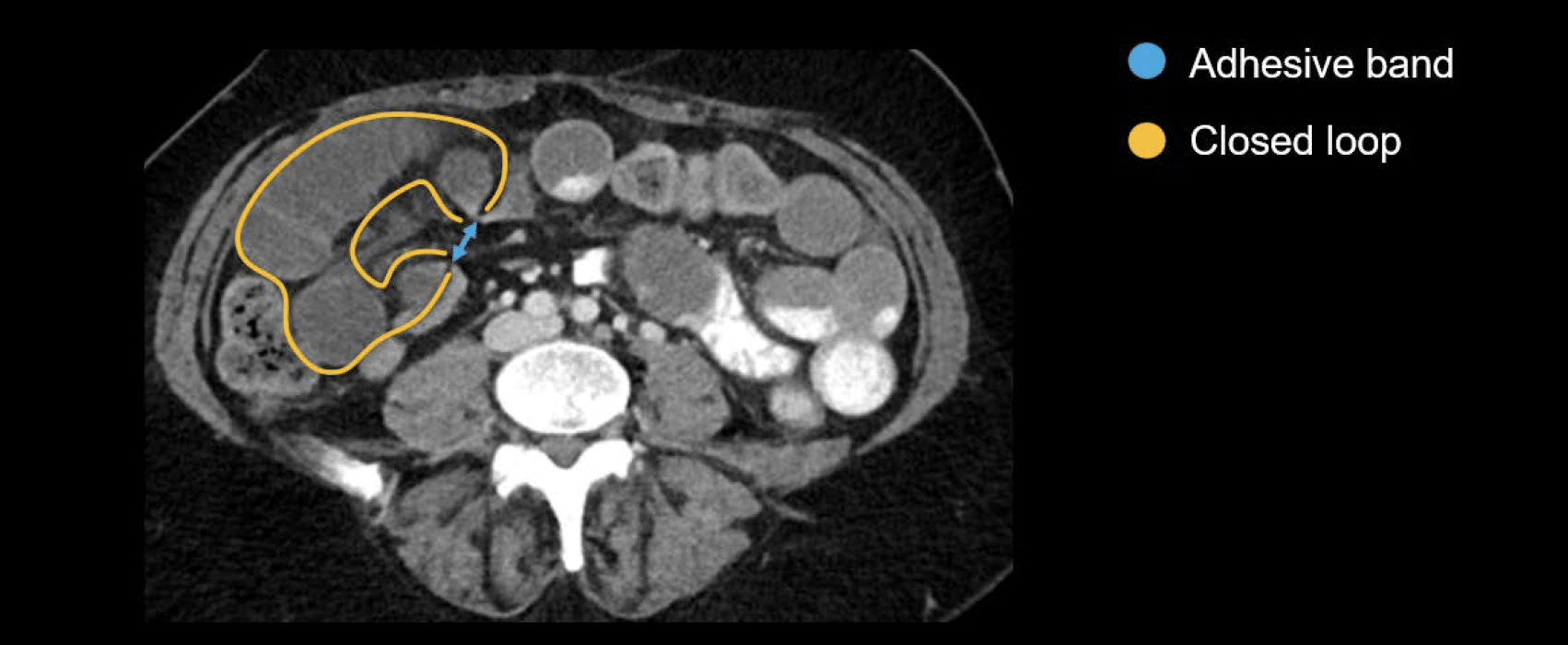
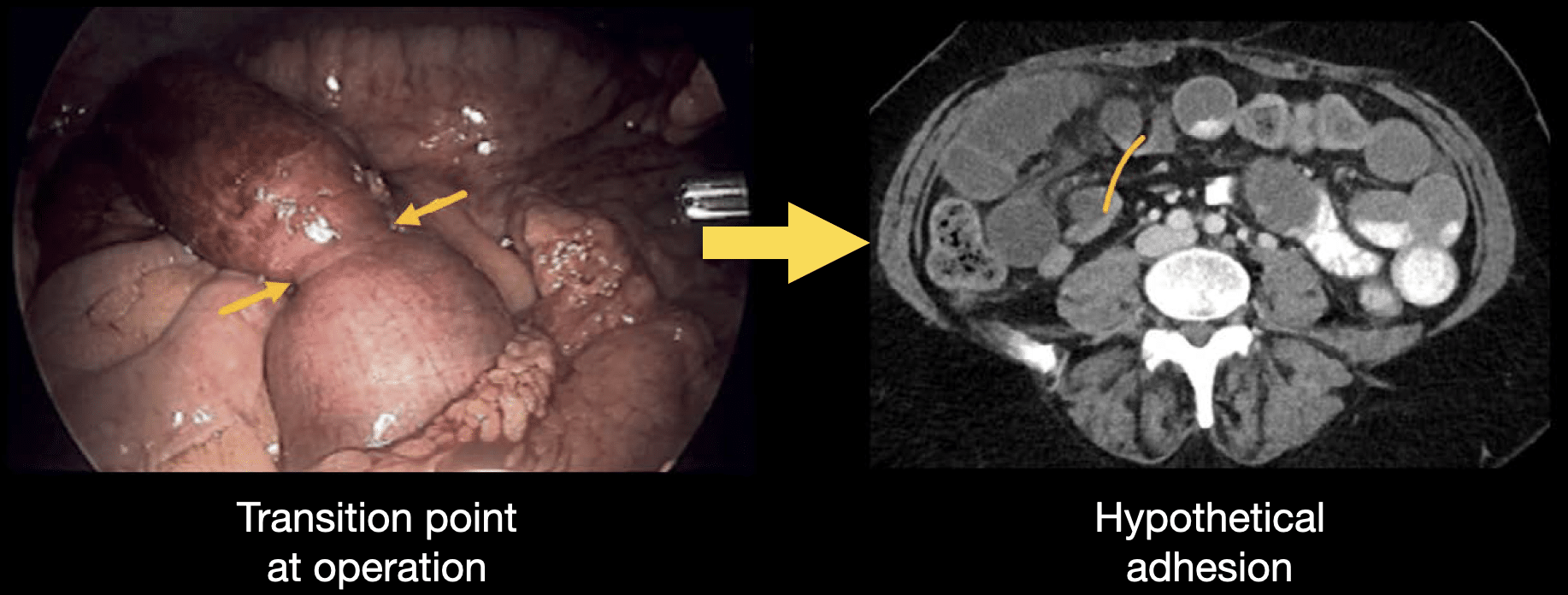
We cannot see adhesive bands on CT; we can only see how they impact the bowel loops. So, we need to combine a bit of imagination with images from surgery to inform our CT interpretation.
Based on an intraoperative image shown, we can postulate the position of the adhesive band on the CT image to help us understand what is causing the bowel to be angulated and narrowed in this case.
Such an obstruction causes the isolated loop to progressively dilate, compressing the vasculature and preventing the small bowel fluid from continuing through the digestive tract. In cases like this, the obstructed segment does not improve with the placing of a nasogastric tube because the tube cannot reach the isolated segment.
Internal hernias
Closed loop obstructions are most commonly caused by adhesions, but internal hernias and volvulus can also lead to these. An internal hernia can be congenital or the result of a surgical defect in the mesentery or omentum that can trap a segment of bowel as the bowel moves through the defect.
Volvulus
A volvulus occurs when there is an abnormal twisting of the bowel. It is commonly associated with congenital malrotation of the bowel but can also be seen in older patients with closed loop obstructions.
Both adhesions and internal hernias can cause volvulus because the bowel in the isolated segment continues to contract and undergo peristalsis during digestion, leading to the twisting of the segment as it progressively dilates.
Diagnosing a closed loop obstruction
There are three key findings that will help you make the diagnosis of closed loop obstruction of the small bowel:
1. Two points of obstruction near each other which create the isolated closed loop segment
The small bowel loops entering and exiting the closed loop will appear sharply angulated (i.e., kinked) and may resemble a bird’s beak, so this is sometimes referred to as the beak sign.

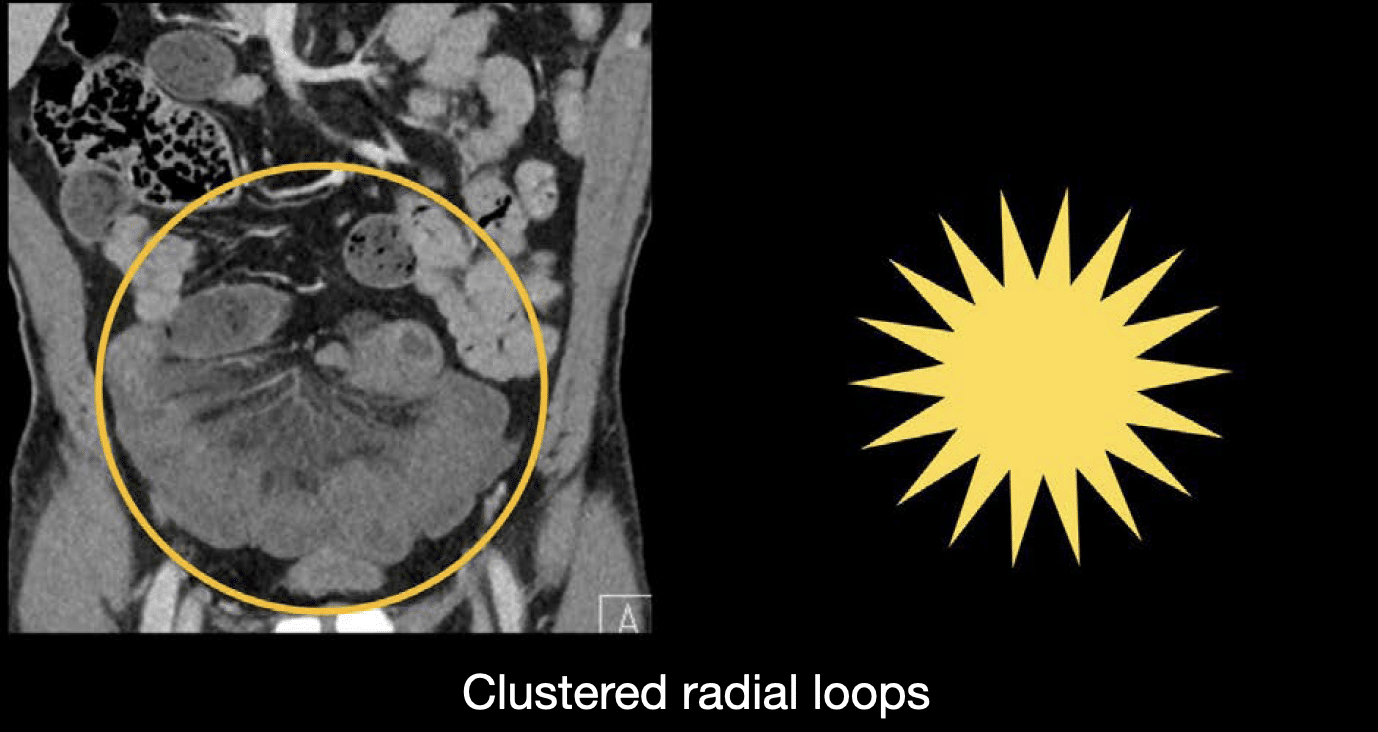
2. A clustered appearance of small bowel in the closed loop with the mesentery and vessels oriented radially toward the point of obstruction
3. Asymmetric oedema and thickening of the closed loop cluster compared to other small bowel loops in the abdomen
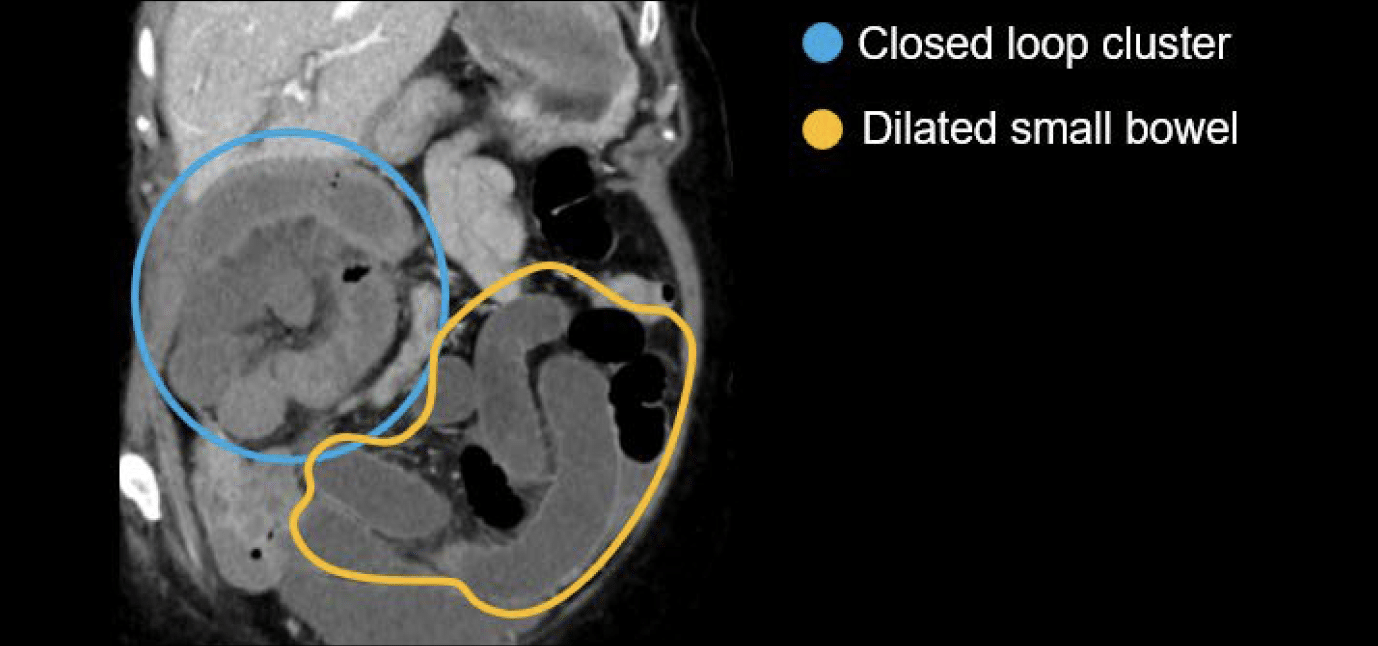
Being able to identify the features of a closed loop segment is particularly important if the small bowel leading into the closed loop is also dilated, as this makes it hard to differentiate the small bowel from the closed loop segment, which may lead you to initially suspect a simple small bowel obstruction only.
Clinical Case 1
Let’s review a case to put our skills into practice. Scroll through the images provided in this online PACS clinical case
- Notice that in this case, it’s clear that oral contrast has been used because, as you scroll inferiorly, you can see it slowly dissolving into the bowel loops that contain fluid. This helps you to know when you are getting closer to the transition point.
- Notice the loop in the right abdomen that looks a little different than the bowel loops on the left. It has a clustered appearance, is slightly more dilated, has surrounding fluid, and mesenteric oedema.
- Follow the upstream bowel into the segment with an angulated transition, and out of that segment through a second angulated transition.
- Notice how both transition points are next to each other. This is a closed loop obstruction so it requires urgent surgical attention!
Clinical Case 2
Let’s review a case to put our skills into practice. Scroll through the images provided in this online PACS clinical case
- Notice that in this case, the proximal bowel is not dilated.
- However, there is no denying that there is a cluster in the lower abdomen that is quite abnormal-looking. It has a radial orientation that really becomes apparent on coronal images, and using all three imaging planes will help you confidently identify these features.
- Notice the asymmetric oedema.
- It’s a little tough to find the transition points, but we can use a tip from the last lesson and look for faecalization. The contents of the loop leading into the closed loop show small bowel faecalization.
- You can also see a sharp angulation – the first transition point.
- Because the loops are surrounded by fluid and have decreased enhancement, they can be hard to follow, but you don’t have to look far to find the second transition point – it is immediately next to the first, defining our closed loop.
This patient was sent to the operating room where the closed loop was found to be caused by an internal hernia.
This is an edited excerpt from the Medmastery course Abdominal CT Pathologies by Michael P. Hartung, MD. Acknowledgement and attribution to Medmastery for providing course transcripts
- Hartung MP. Abdominal CT: Common Pathologies. Medmastery
- Hartung MP. Abdominal CT: Essentials. Medmastery
- Hartung MP. Abdomen CT: Trauma. Medmastery
References
- Hartung MP. Abdominal CT: Imaging the small bowel
- Nickson C. Small bowel obstruction DDx. CCC
- Cadogan M. AXR Interpretation. CCC
- Nickson C. Abdominal X-ray and CT. CCC
- Top 100 CT scan quiz. LITFL
Radiology Library: Abdominal CT: Imaging important abdominal structures
- Hartung MP. Abdominal CT: acute appendicitis
- Hartung MP. Abdominal CT: diverticulitis
- Hartung MP. Abdominal CT: small bowel obstruction
- Hartung MP. Abdominal CT: closed loop small bowel obstruction
- Hartung MP. Abdominal CT: enteritis and colitis
- Hartung MP. Abdominal CT: peptic ulcer disease
- Hartung MP. Abdominal CT: peptic ulcer perforation
- Hartung MP. Abdominal CT: bowel perforation
Abdominal CT interpretation

Assistant Professor of Abdominal Imaging and Intervention at the University of Wisconsin Madison School of Medicine and Public Health. Interests include resident and medical student education, incorporating the latest technology for teaching radiology. I am also active as a volunteer teleradiologist for hospitals in Peru and Kenya. | Medmastery | Radiopaedia | Website | Twitter | LinkedIn | Scopus

MBChB (hons), BMedSci - University of Edinburgh. Living the good life in emergency medicine down under. Interested in medical imaging and physiology. Love hiking, cycling and the great outdoors.