![]()
Abdominal CT: peptic ulcer disease
Recognising peptic ulcer disease
A peptic ulcer is a sore in the inner lining of the stomach or duodenum usually caused by inflammation or infection. Patients with peptic ulcer disease often present with epigastric or upper abdominal pain.
Major risk factors include:
- Frequent use of nonsteroidal anti-inflammatory drugs (NSAIDs)
- Helicobacter pylori (H. pylori) infection
- Regular consumption of alcohol
- Smoking
The most common locations for ulcers to form are in the stomach or duodenum.
A peptic ulcer can affect every layer of the digestive tract forming a hole (i.e., perforation) which allows the gastric or enteric contents to leak into the abdominal cavity. This results in severe abdominal pain, leukocytosis, and peritonitis on physical examination
Key findings
CT is excellent for making the diagnosis of a perforated ulcer and can help guide treatment. However, the ulcer crater itself can be difficult to directly see on CT. Often you are looking for secondary signs of inflammation:
- Mucosal hyperenhancement
- Thickening and swelling of the bowel wall
- Surrounding stranding
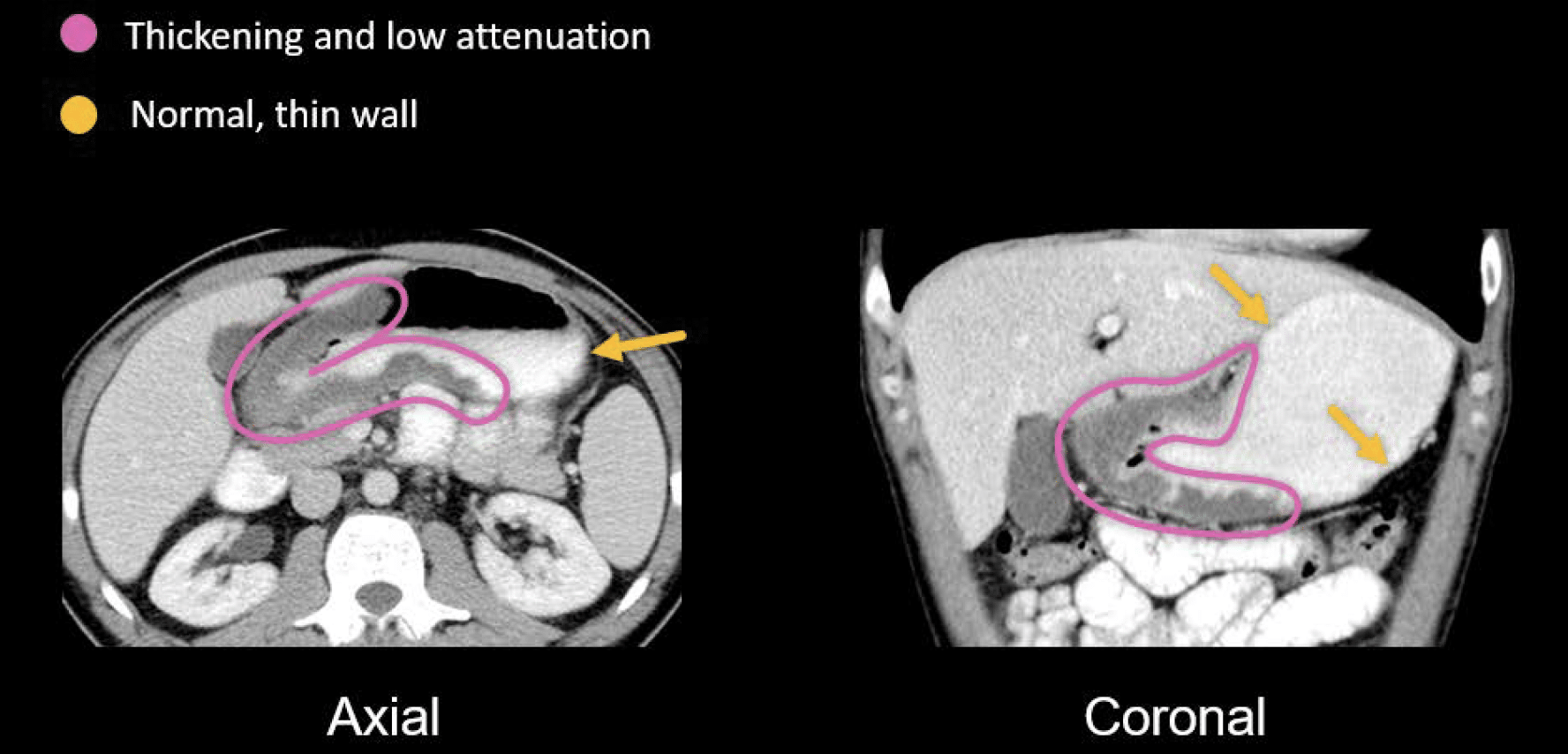
Example
There is an impressive thickening of the gastric antrum and pylorus with relatively low attenuation of the wall, indicating oedema. You can compare this to the thin wall of the gastric body.
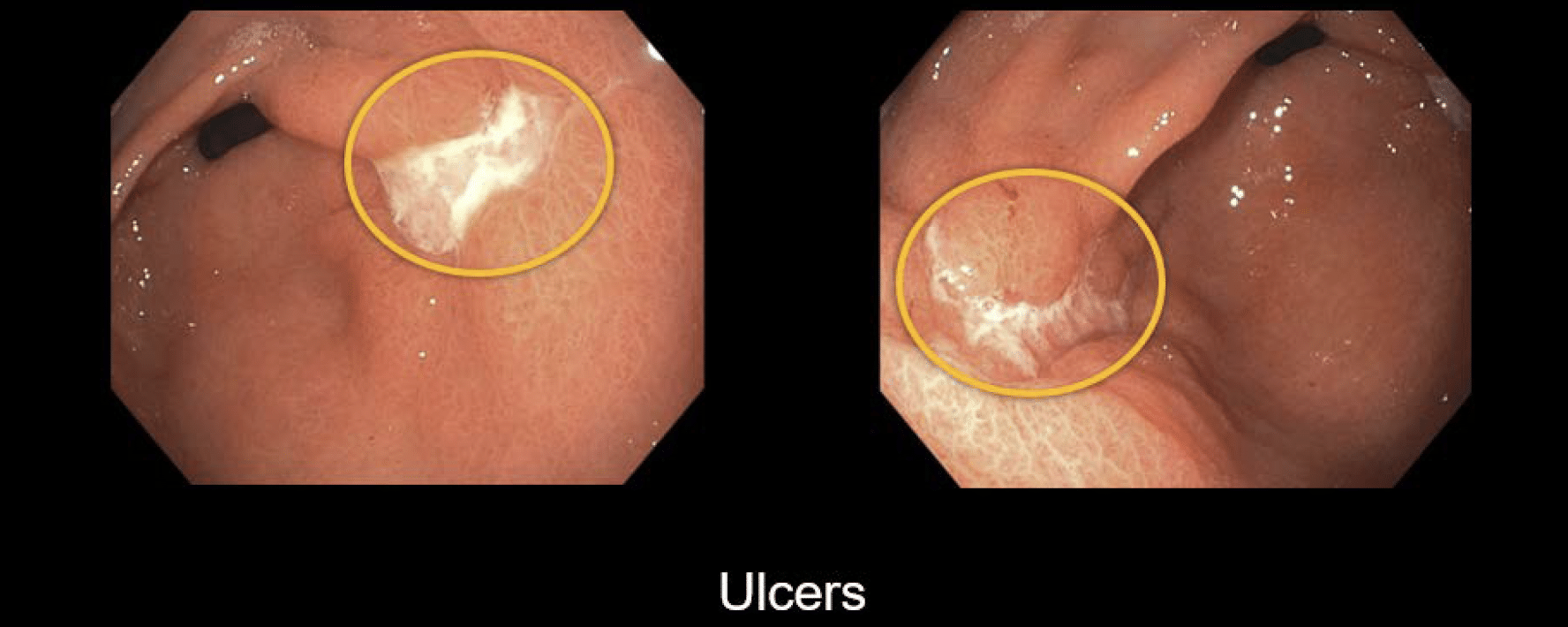
Based on the concern for ulcers after viewing this patient’s CT, the patient underwent an endoscopy to look at the upper GI tract where several gastric ulcers were identified. Below, the ulcers are the white-looking areas that contrast the normal, smooth, pink mucosal lining of the stomach.
Clinical Case 1
Scroll through these images from a patient to take a look at an ulcer using a PACS viewer
- Ulcers can form deeper craters that are at risk for perforation. In this example, you can see an ulcer crater arising from the duodenal bulb.
- To find the ulcer, follow the upper GI tract to the bulb.
- Notice the mushroom-like shape and how the surrounding fat and soft tissues have stranding and look inflamed
Because this ulcer has not perforated, it will most likely be managed medically, although the patient should be carefully followed clinically as the ulcer is certainly at risk for perforation.
This is an edited excerpt from the Medmastery course Abdominal CT Pathologies by Michael P. Hartung, MD. Acknowledgement and attribution to Medmastery for providing course transcripts
- Hartung MP. Abdominal CT: Common Pathologies. Medmastery
- Hartung MP. Abdominal CT: Essentials. Medmastery
- Hartung MP. Abdomen CT: Trauma. Medmastery
References
- Hartung MP. Abdominal CT: Imaging the small bowel
- Nickson C. Small bowel obstruction DDx. CCC
- Cadogan M. AXR Interpretation. CCC
- Nickson C. Abdominal X-ray and CT. CCC
- Top 100 CT scan quiz. LITFL
Radiology Library: Abdominal CT: Imaging important abdominal structures
- Hartung MP. Abdominal CT: acute appendicitis
- Hartung MP. Abdominal CT: diverticulitis
- Hartung MP. Abdominal CT: small bowel obstruction
- Hartung MP. Abdominal CT: closed loop small bowel obstruction
- Hartung MP. Abdominal CT: enteritis and colitis
- Hartung MP. Abdominal CT: peptic ulcer disease
- Hartung MP. Abdominal CT: peptic ulcer perforation
- Hartung MP. Abdominal CT: bowel perforation
Abdominal CT interpretation

Assistant Professor of Abdominal Imaging and Intervention at the University of Wisconsin Madison School of Medicine and Public Health. Interests include resident and medical student education, incorporating the latest technology for teaching radiology. I am also active as a volunteer teleradiologist for hospitals in Peru and Kenya. | Medmastery | Radiopaedia | Website | Twitter | LinkedIn | Scopus

MBChB (hons), BMedSci - University of Edinburgh. Living the good life in emergency medicine down under. Interested in medical imaging and physiology. Love hiking, cycling and the great outdoors.