
![]()
Abdominal CT: enteritis and colitis
Identifying enteritis and colitis
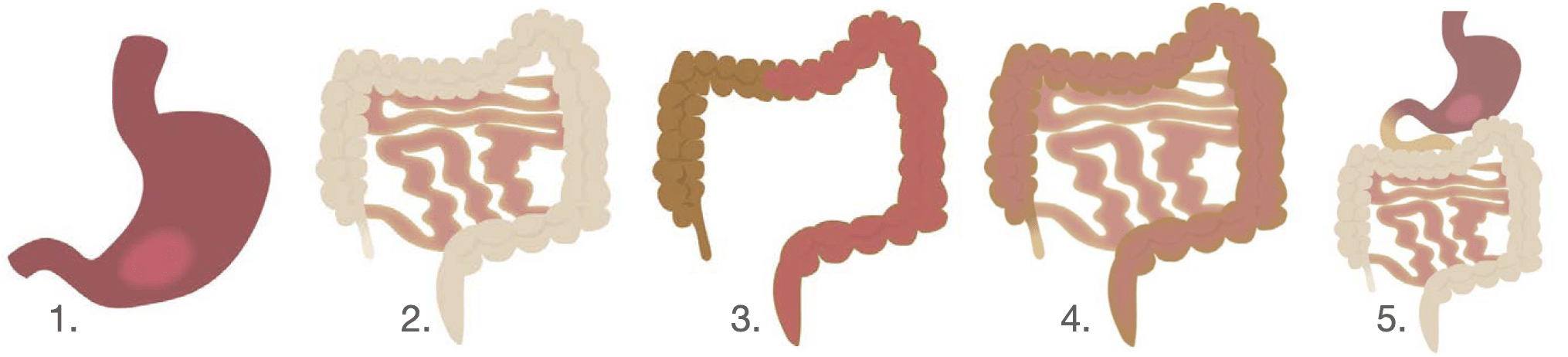
We review the most common presentations of gastrointestinal tract inflammation that do not require surgery. In terms of inflammation:
- Gastritis is inflammation of the stomach.
- Enteritis involves the small bowel.
- Colitis involves the large bowel
- Enterocolitis involves the small and large bowel.
- Gastroenteritis includes the stomach and small bowel.
Inflammation of the gastrointestinal tract can be caused by different factors, including:
- Infection
- Inflammatory disorders e.g. inflammatory bowel disease
- Ischaemia
Key findings
Depending on the nature of the inflammation, you might see abnormalities in the layers of the bowel wall (including the innermost mucosa, the middle submucosal and muscular layers, and the outer wall, or serosa).
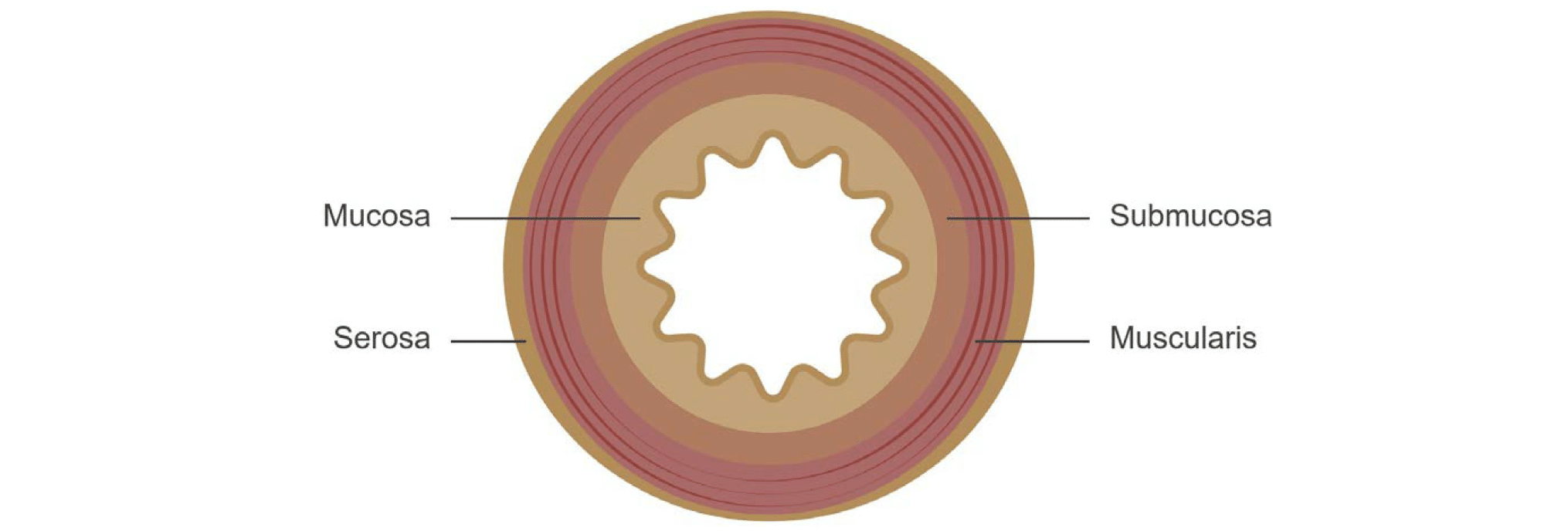
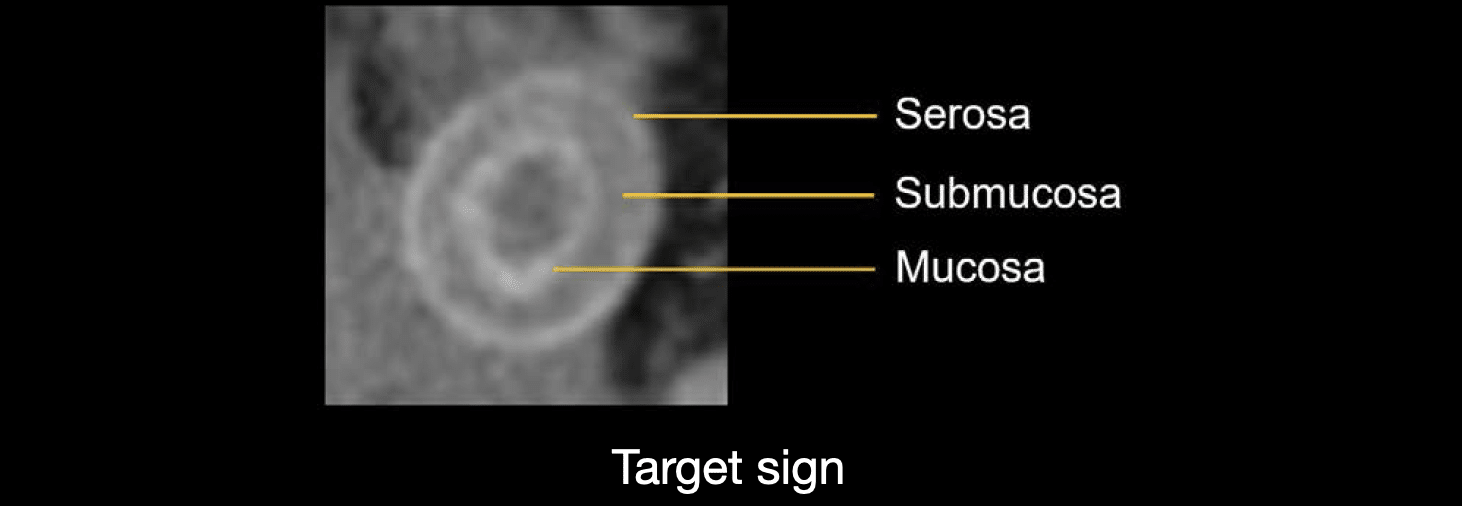
Often you will see increased enhancement of the inner mucosal lining, edema in the middle layers, and even increased enhancement of the serosa. This pattern of enhancement of the bowel wall resembles a target.
Diagnosing GI tract inflammation
When the gastrointestinal tract becomes inflamed, there are three primary indicators to look for:
- Increased thickness of the bowel wall
- Areas of increased or decreased enhancement
- Surrounding fluid or stranding in the mesenteric fat

Clinical examples
Enteritis
If we look at the jejunum of a normal small bowel, it has a characteristic feathery fold pattern, whereas the ileum has a thin and relatively featureless wall that looks like a single enhancing line. Notice in the case of enteritis we can differentiate the layers of the wall due to abnormal thickening and enhancement.

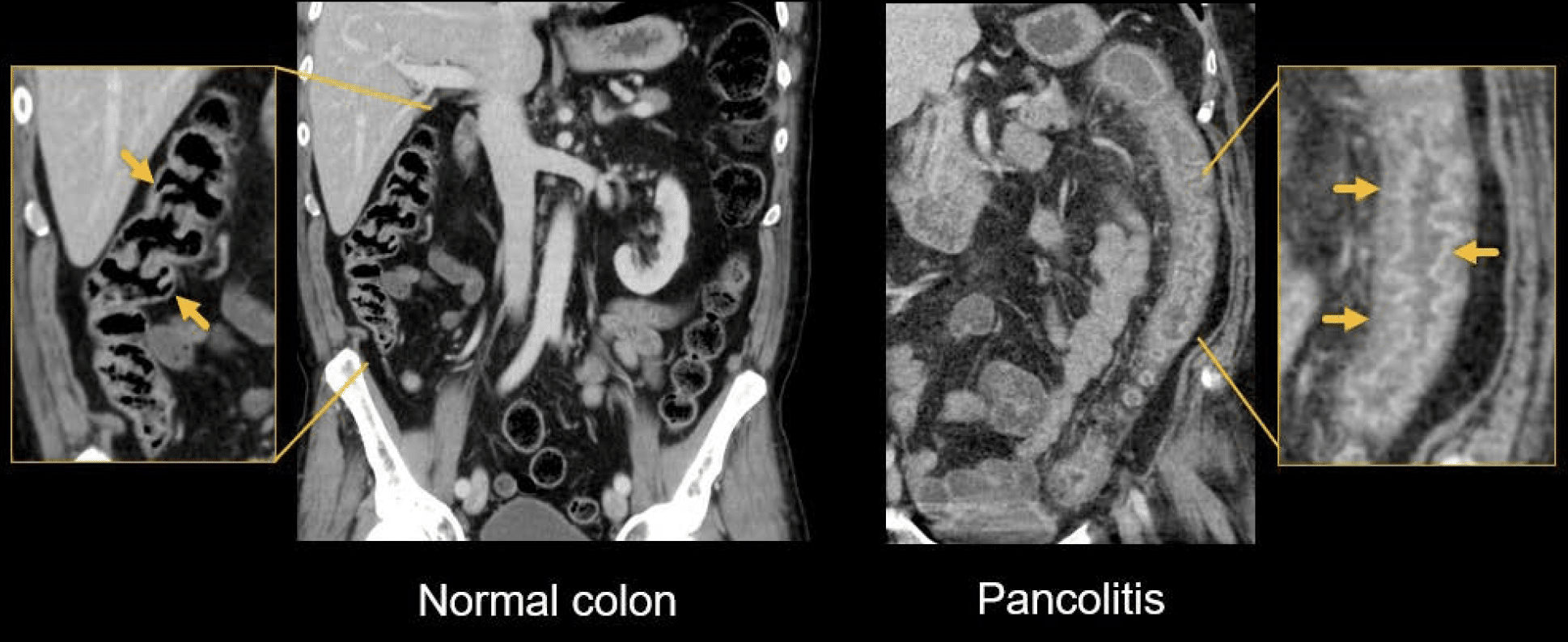
Pancolitis
The normal colon wall appears as a relatively thin line. With pancolitis, however, you can see differentiation of the bowel wall layers within the thickened wall.
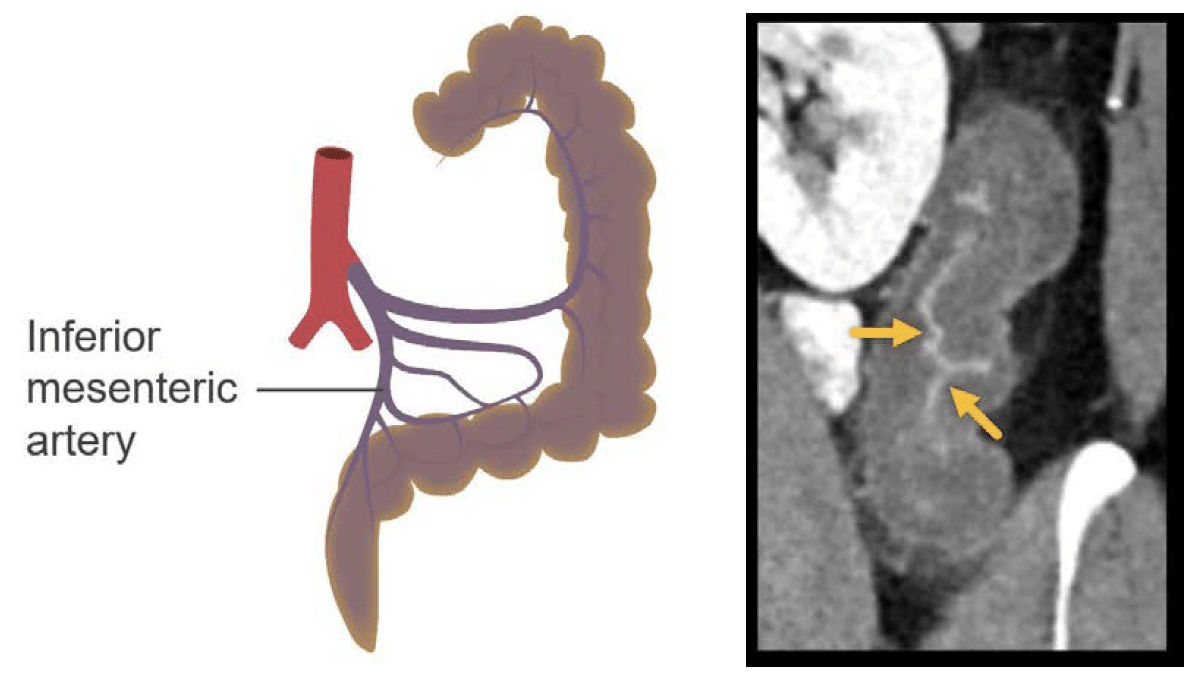
Ischaemic colitis
Decreased blood flow to the colon results in injury and inflammation of the wall. Usually, this is not due to blockage of the artery, but rather to a temporary decrease in blood flow. The pattern shown on this CT corresponds to a common presentation that follows the distribution of a specific artery – the inferior mesenteric artery.
Clinical Case 1
Scroll through the images from a patient who presented with abdominal pain, nausea, diarrhoea, and an elevated white blood cell count.
- Note that there is clinical suspicion of an infection of the GI tract.
- As you scroll the images and focus your evaluation on the GI, you may find it particularly helpful to use the coronal images. Coronal images cover so much territory of the GI tract in each image, which helps you to get a global picture of what is going on.
- In this case, you can notice a mildly dilated and thickened small bowel in the right lower quadrant, which corresponds to the ileum.
- Notice also that there is some associated fluid / stranding involving these loops.
- You can also see thickening and increased mucosal enhancement of the entire colon. This pattern is typical for enterocolitis due to infection.
Clinical Case 2
Scroll through these images from a patient who presented with abdominal pain, and bloody, diarrhoea.
- The small bowel is normal in this case, as is much of the colon.
- However, from the splenic flexure down through the sigmoid colon, notice how the small bowel is quite thickened with increased fluid in the middle layer and increased enhancement of the inner mucosal and outer serosal layers.
- This is a typical appearance and distribution for ischaemic colitis due to temporarily decreased blood flow to the colon along the distribution of the inferior mesenteric artery.
This is an edited excerpt from the Medmastery course Abdominal CT Pathologies by Michael P. Hartung, MD. Acknowledgement and attribution to Medmastery for providing course transcripts
- Hartung MP. Abdominal CT: Common Pathologies. Medmastery
- Hartung MP. Abdominal CT: Essentials. Medmastery
- Hartung MP. Abdomen CT: Trauma. Medmastery
References
- Hartung MP. Abdominal CT: Imaging the small bowel
- Nickson C. Small bowel obstruction DDx. CCC
- Cadogan M. AXR Interpretation. CCC
- Nickson C. Abdominal X-ray and CT. CCC
- Top 100 CT scan quiz. LITFL
Radiology Library: Abdominal CT: Imaging important abdominal structures
- Hartung MP. Abdominal CT: acute appendicitis
- Hartung MP. Abdominal CT: diverticulitis
- Hartung MP. Abdominal CT: small bowel obstruction
- Hartung MP. Abdominal CT: closed loop small bowel obstruction
- Hartung MP. Abdominal CT: enteritis and colitis
- Hartung MP. Abdominal CT: peptic ulcer disease
- Hartung MP. Abdominal CT: peptic ulcer perforation
- Hartung MP. Abdominal CT: bowel perforation
Abdominal CT interpretation

Assistant Professor of Abdominal Imaging and Intervention at the University of Wisconsin Madison School of Medicine and Public Health. Interests include resident and medical student education, incorporating the latest technology for teaching radiology. I am also active as a volunteer teleradiologist for hospitals in Peru and Kenya. | Medmastery | Radiopaedia | Website | Twitter | LinkedIn | Scopus

MBChB (hons), BMedSci - University of Edinburgh. Living the good life in emergency medicine down under. Interested in medical imaging and physiology. Love hiking, cycling and the great outdoors.