
![]()
Abdominal CT: peptic ulcer perforation
Spotting a peptic ulcer perforation
While many ulcers can be managed medically, perforated ulcers (i.e., ulcers that form a hole through the bowel wall) require surgical intervention. So, let’s spend some time highlighting the key findings that raise suspicion of perforation.
Key findings
- Air pockets outside the bowel wall
- Fluid outside the bowel wall
- Inflammation
The first sign of perforation you will probably notice is pockets of air outside of the bowel wall and throughout the abdominal cavity. These pockets can have a range of appearances, from large pockets in the anterior abdomen to a few small dots (i.e., locules) of air near the site of perforation.
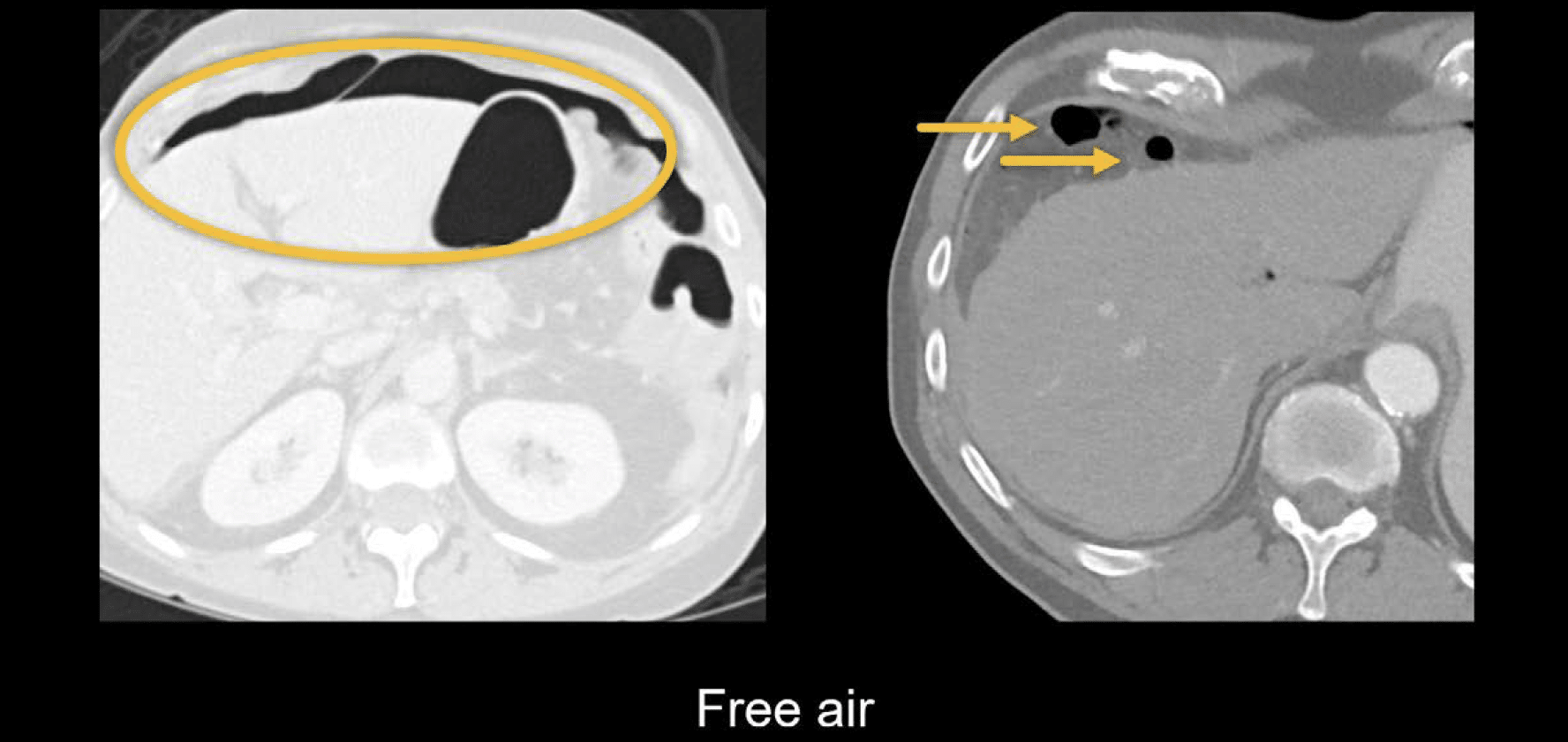
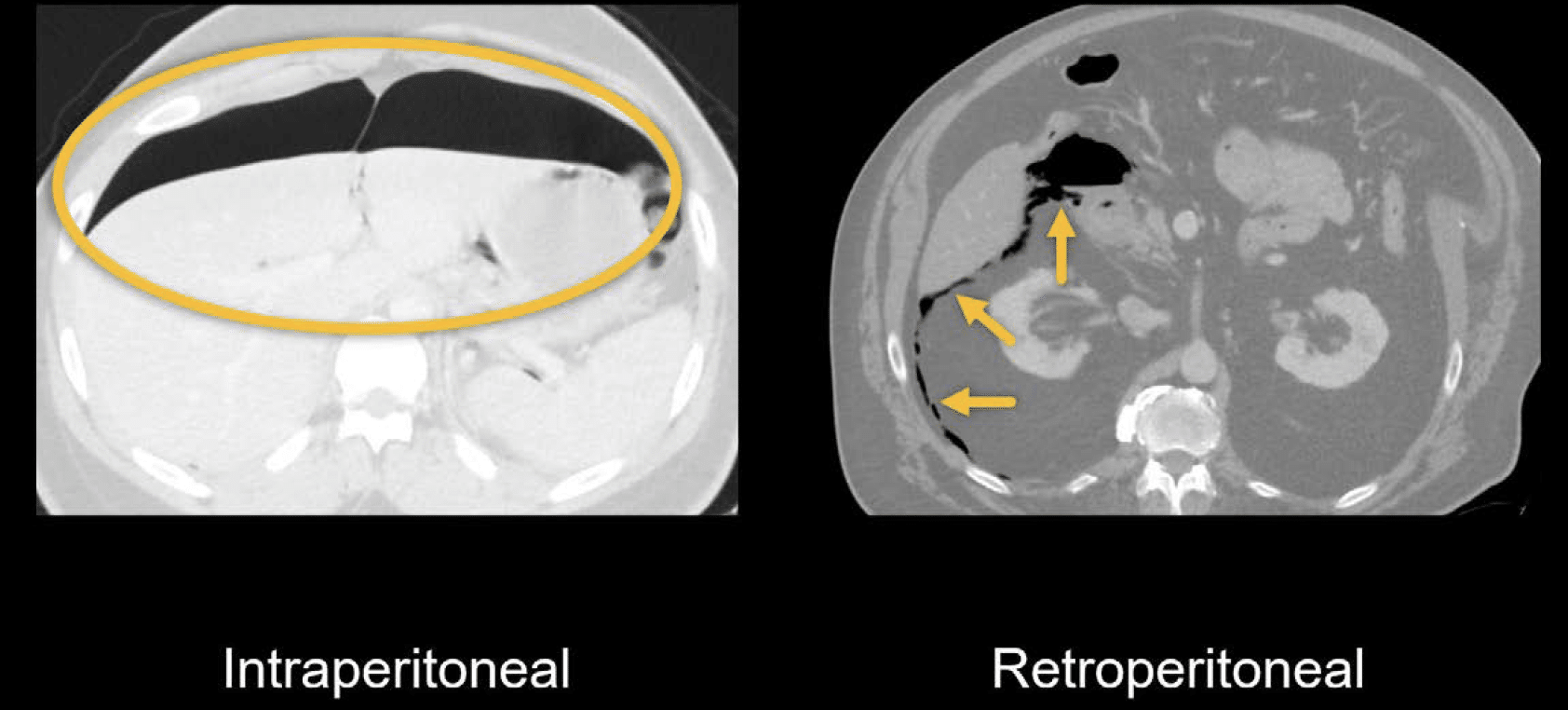
After perforation of the stomach and duodenal bulb, air can travel freely within the peritoneum. We call this intraperitoneal air. Air can also travel behind the peritoneum, called retroperitoneal air. This can occur with perforation of the second or third portions of the duodenum.
Clinical examples
In each of these cases, the pattern of fluid, air, and inflammation help to locate the source of perforation.
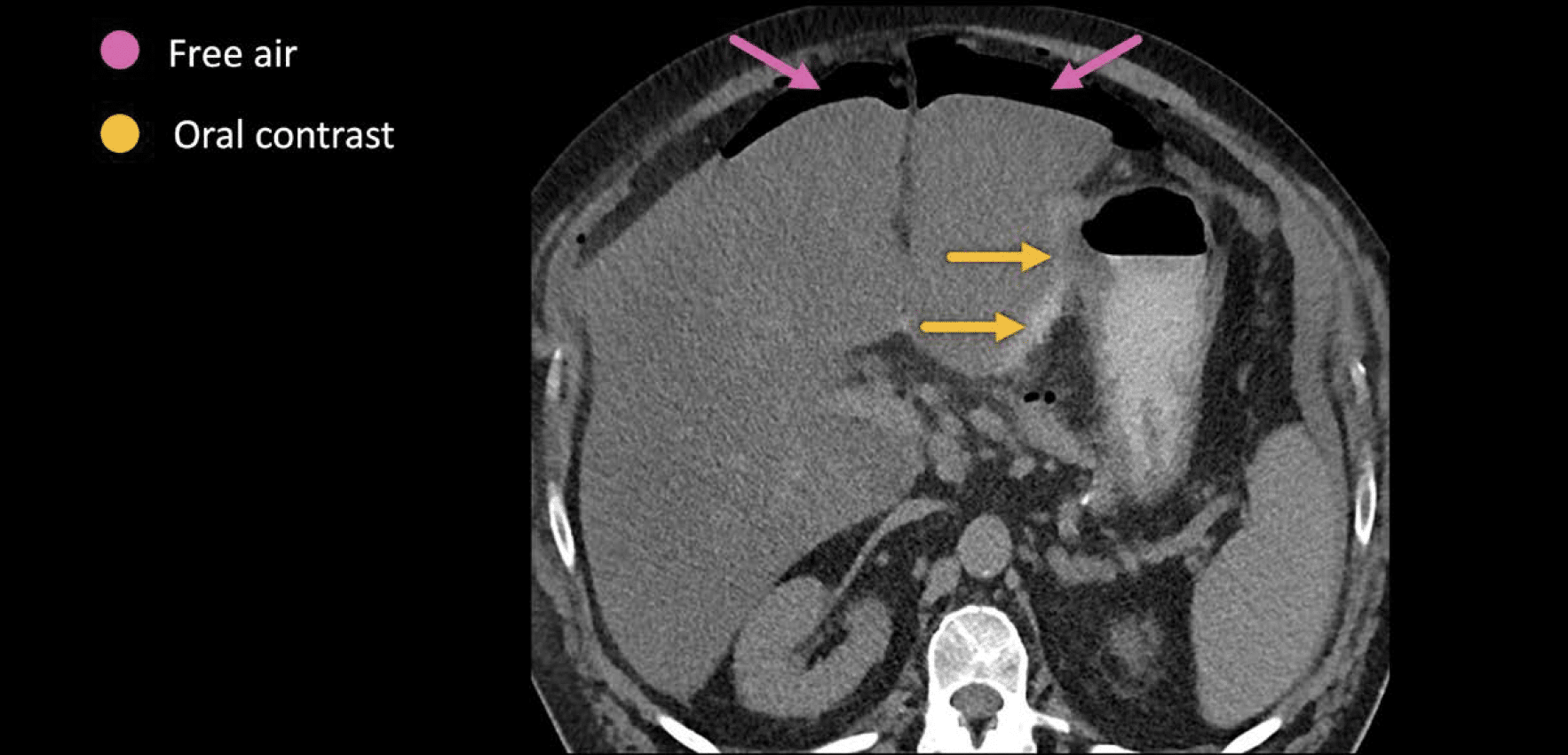
Example 1
This CT demonstrates shows two key findings following perforation – oral contrast leaking out from the bowel and around the left edge of the liver, and free air in the anterior abdomen along the front of the liver.
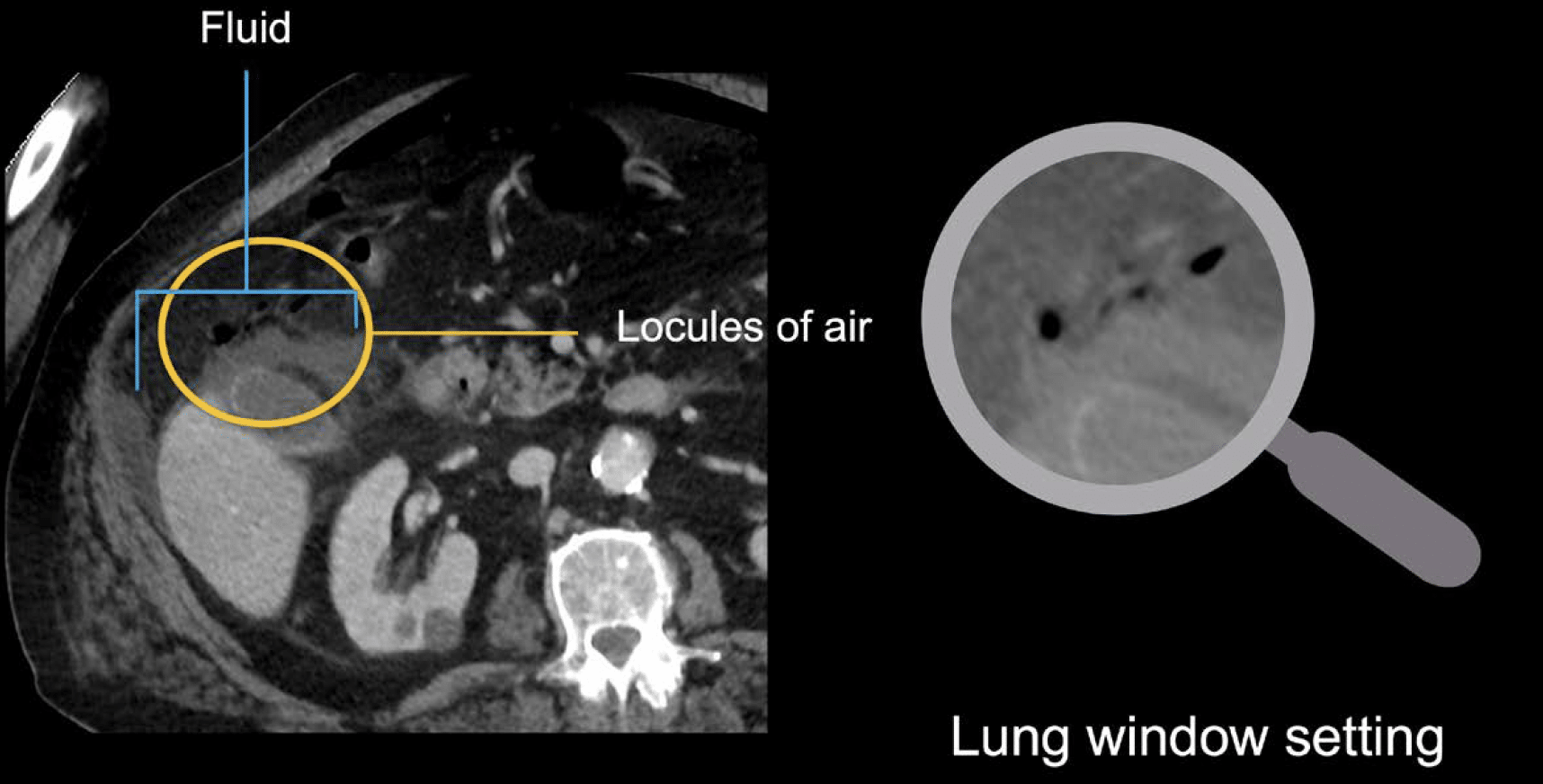
Example 2
This CT demonstrates fluid around the lower margin of the liver and gallbladder with a few small surrounding dots of air, which are best seen using lung window settings. Fluid and small locules of air in this location suggest a gastric or duodenal source of perforation.
In some cases, the site of perforation can be relatively subtle on CT. However, if the patient is able to even drink a small amount, oral contrast can help to highlight the ulcer or show the site of leakage. Carefully running through the stomach and duodenum on both axial and coronal images will usually lead you to the site of perforation.
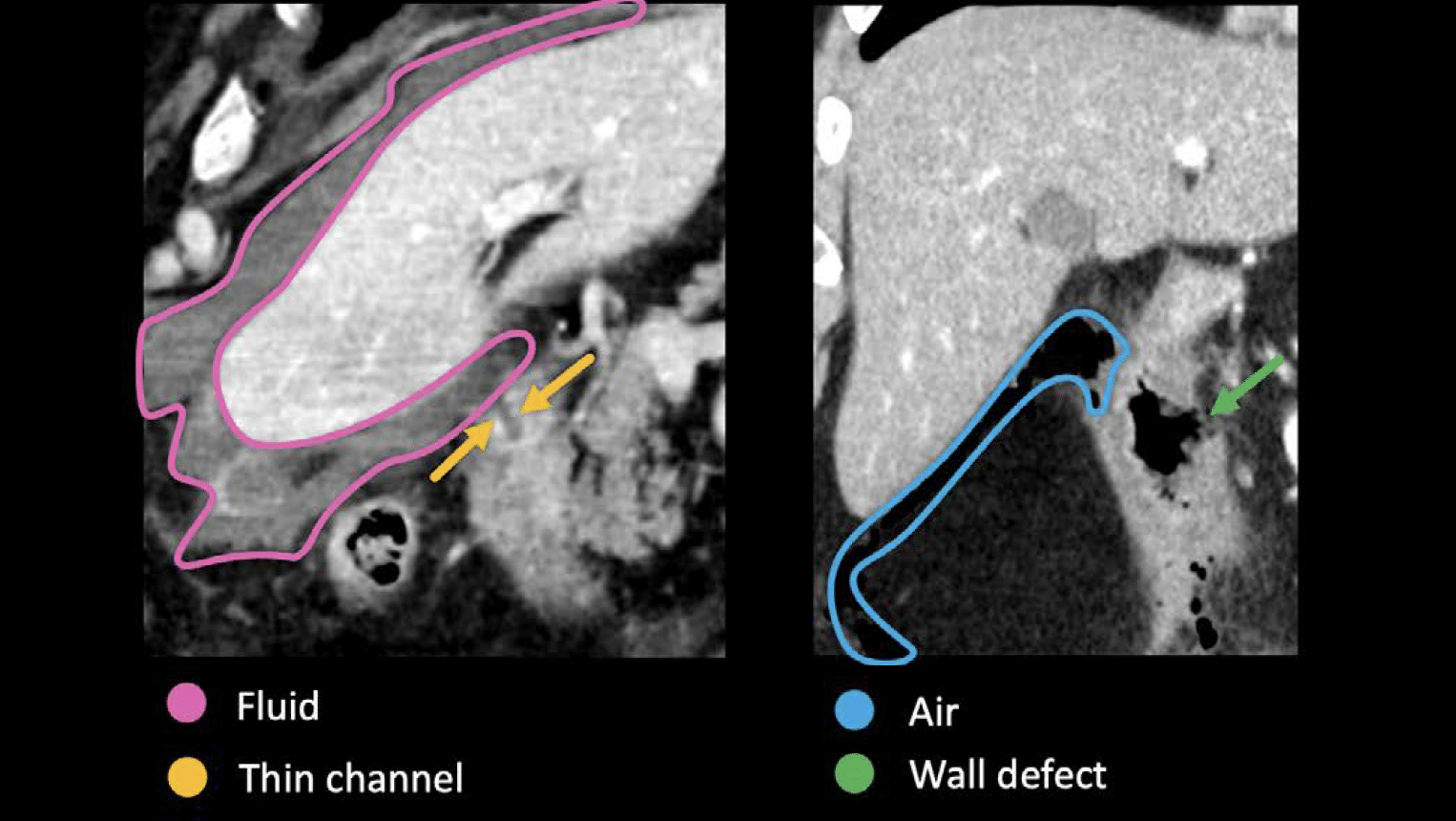
Example 3, 4
Two peptic ulcer perforation cases.
- Left: subtle example with a thin channel through the duodenal wall, resulting in fluid extending around the liver.
- Right: more obvious perforation – a wall defect with air extending outside of the bowel along the undersurface of the liver.
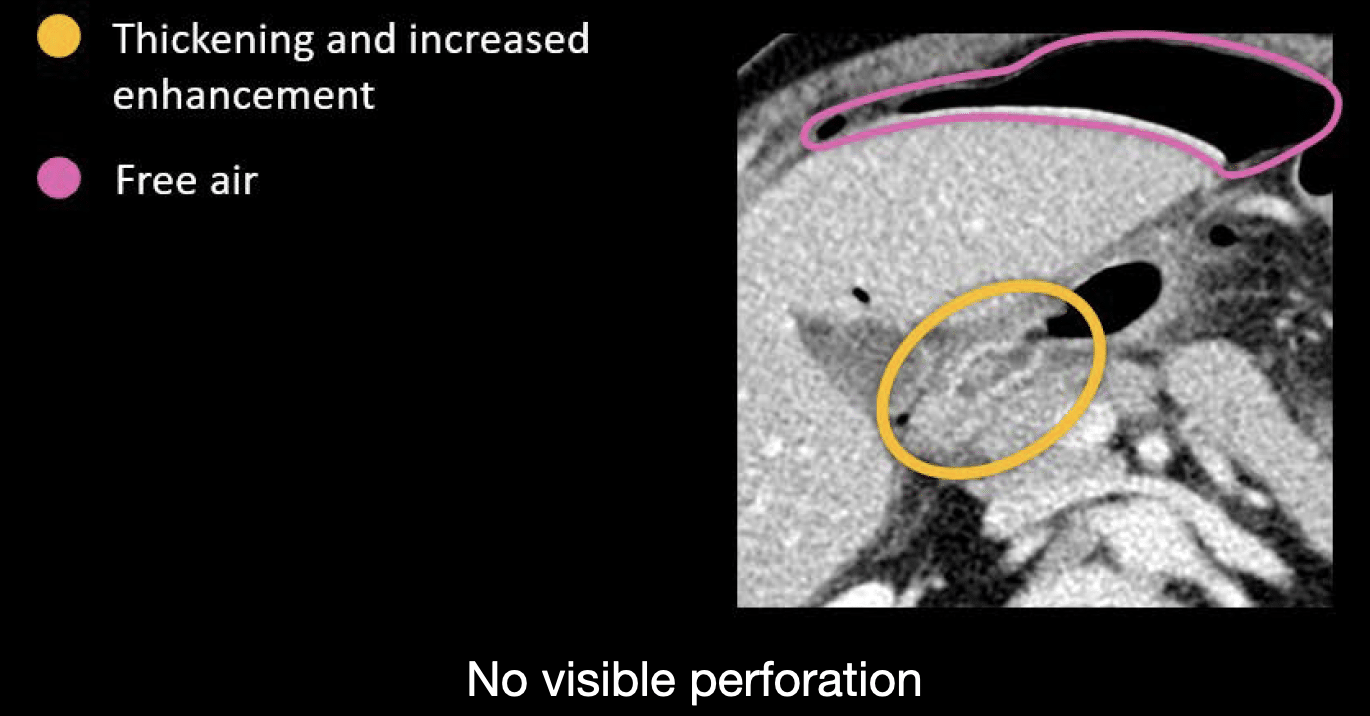
Example 5
CT demonstrates thickening and increased enhancement of the duodenal bulb indicating inflammation related to an ulcer, but we cannot see an obvious site of perforation this time. However, we know a perforation has occurred because of the free air in front of the liver.
Clinical Case 1
Scroll through these images from a patient presenting with severe abdominal pain.
- Switching on lung windows, the first thing you might notice is free air. There are several small locules in front of the liver, in the hepatic hilum, and in the left upper quadrant. This indicates that a perforation has occurred.
- Going back to soft tissue windows, notice there is fluid and stranding as well, mostly in the right upper quadrant.
- This pattern of free air and fluid is highly suggestive of a duodenal ulcer, so run the upper GI tract carefully.
- Notice that there is oral contrast in the stomach and proximal small bowel. 5. You can see a defect in the lateral wall of the duodenum.
- On coronal sections, there is a thin stream of contrast flowing out from the defect along the lower margin of the gallbladder. This is the site of perforation.
- The oral contrast can help you to confidently identify the location, which will be used to guide surgical management.
This is an edited excerpt from the Medmastery course Abdominal CT Pathologies by Michael P. Hartung, MD. Acknowledgement and attribution to Medmastery for providing course transcripts
- Hartung MP. Abdominal CT: Common Pathologies. Medmastery
- Hartung MP. Abdominal CT: Essentials. Medmastery
- Hartung MP. Abdomen CT: Trauma. Medmastery
References
- Hartung MP. Abdominal CT: Imaging the small bowel
- Nickson C. Small bowel obstruction DDx. CCC
- Cadogan M. AXR Interpretation. CCC
- Nickson C. Abdominal X-ray and CT. CCC
- Top 100 CT scan quiz. LITFL
Radiology Library: Abdominal CT: Imaging important abdominal structures
- Hartung MP. Abdominal CT: acute appendicitis
- Hartung MP. Abdominal CT: diverticulitis
- Hartung MP. Abdominal CT: small bowel obstruction
- Hartung MP. Abdominal CT: closed loop small bowel obstruction
- Hartung MP. Abdominal CT: enteritis and colitis
- Hartung MP. Abdominal CT: peptic ulcer disease
- Hartung MP. Abdominal CT: peptic ulcer perforation
- Hartung MP. Abdominal CT: bowel perforation
Abdominal CT interpretation

Assistant Professor of Abdominal Imaging and Intervention at the University of Wisconsin Madison School of Medicine and Public Health. Interests include resident and medical student education, incorporating the latest technology for teaching radiology. I am also active as a volunteer teleradiologist for hospitals in Peru and Kenya. | Medmastery | Radiopaedia | Website | Twitter | LinkedIn | Scopus

MBChB (hons), BMedSci - University of Edinburgh. Living the good life in emergency medicine down under. Interested in medical imaging and physiology. Love hiking, cycling and the great outdoors.
