![]()
Abdominal CT: small bowel obstruction
Diagnosing small bowel obstruction
Small bowel obstruction occurs when there is a blockage of the small intestine, which causes dilation of the bowel proximal to the blockage.
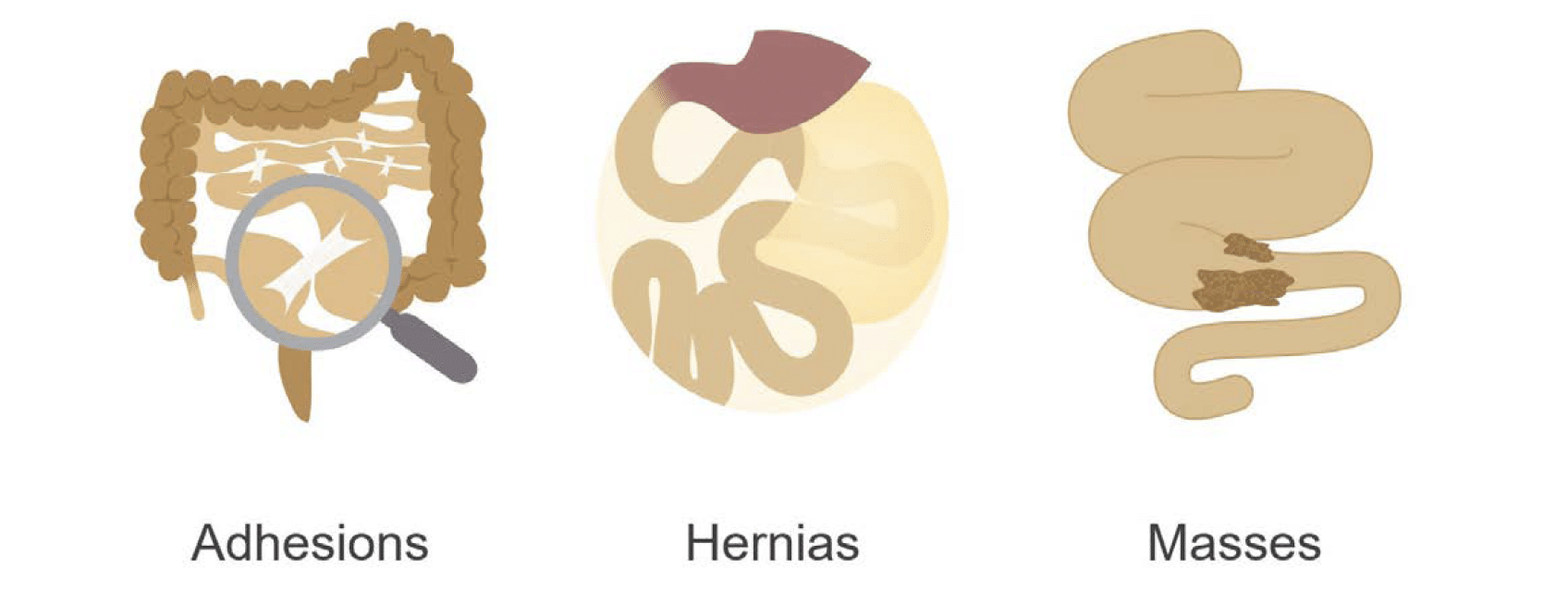
Blockages are most commonly associated with
- Adhesion – scar tissue in the abdomen
- Hernias – bowel escapes into places that it should not be…
- Masses – benign or malignant
Signs and symptoms
Patients with small bowel obstruction typically present with nausea, vomiting, central abdominal pain and distension
Imaging and treatment
The role of CT in these cases is to identify the cause of the obstruction and to look for complications such as restricted blood supply or perforation that might require urgent surgery.
Ultimately, many of these patients can be successfully managed non-operatively with a nasogastric tube, which goes from the nose to the stomach to remove excess fluid, giving the bowel a chance to rest. More severe or complex cases may require surgery, and for this reason, every case requires a thorough imaging review to avoid delays in care.
Note: A scout image is the planning x-ray that the CT scanner uses to determine which part of the body to scan. These images are often helpful in the setting of obstruction because they provide us with an idea of how things look on an x-ray, and they can be compared to follow-up x-rays if the patient undergoes conservative management with nasogastric tube placement and bowel rest.
Small bowel obstruction
In typical small bowel obstruction caused by adhesive disease there are three key imaging findings to help make the diagnosis:
- Dilated, fluid-filled loops of small bowel
- Transition point
- Faecalization
Dilated, fluid-filled loops of small bowel.
The degree of dilation can vary based on the severity and acuity of the obstruction but, in general, when the small bowel loops are greater than 2.5 – 3cm in diameter, an obstruction becomes likely.
Note: It is helpful to remember that normal small bowel may have some fluid, or even a slightly dilated loop or two. However, normal small bowel does not have that tense, crowded appearance of many dilated loops as is seen with an obstruction.

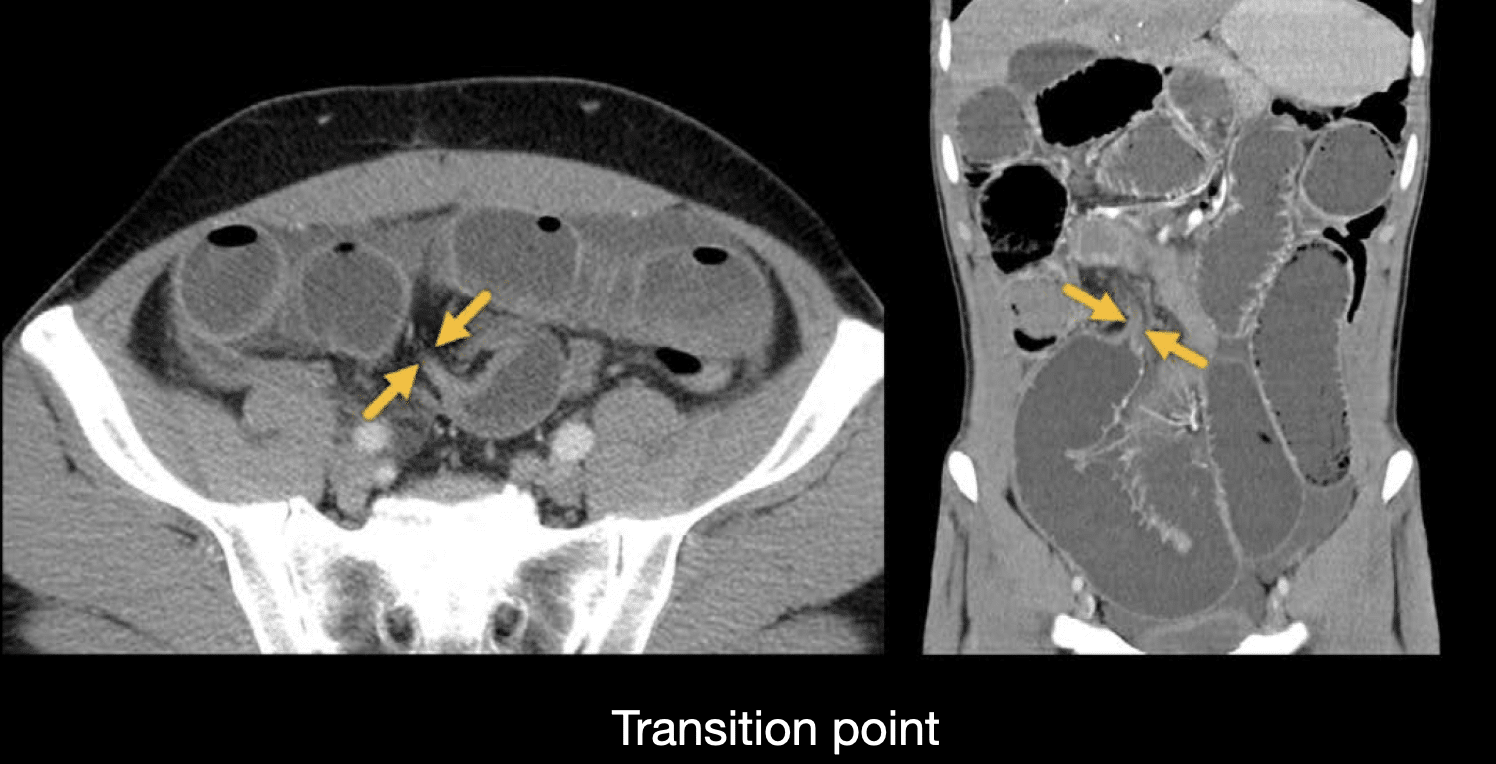
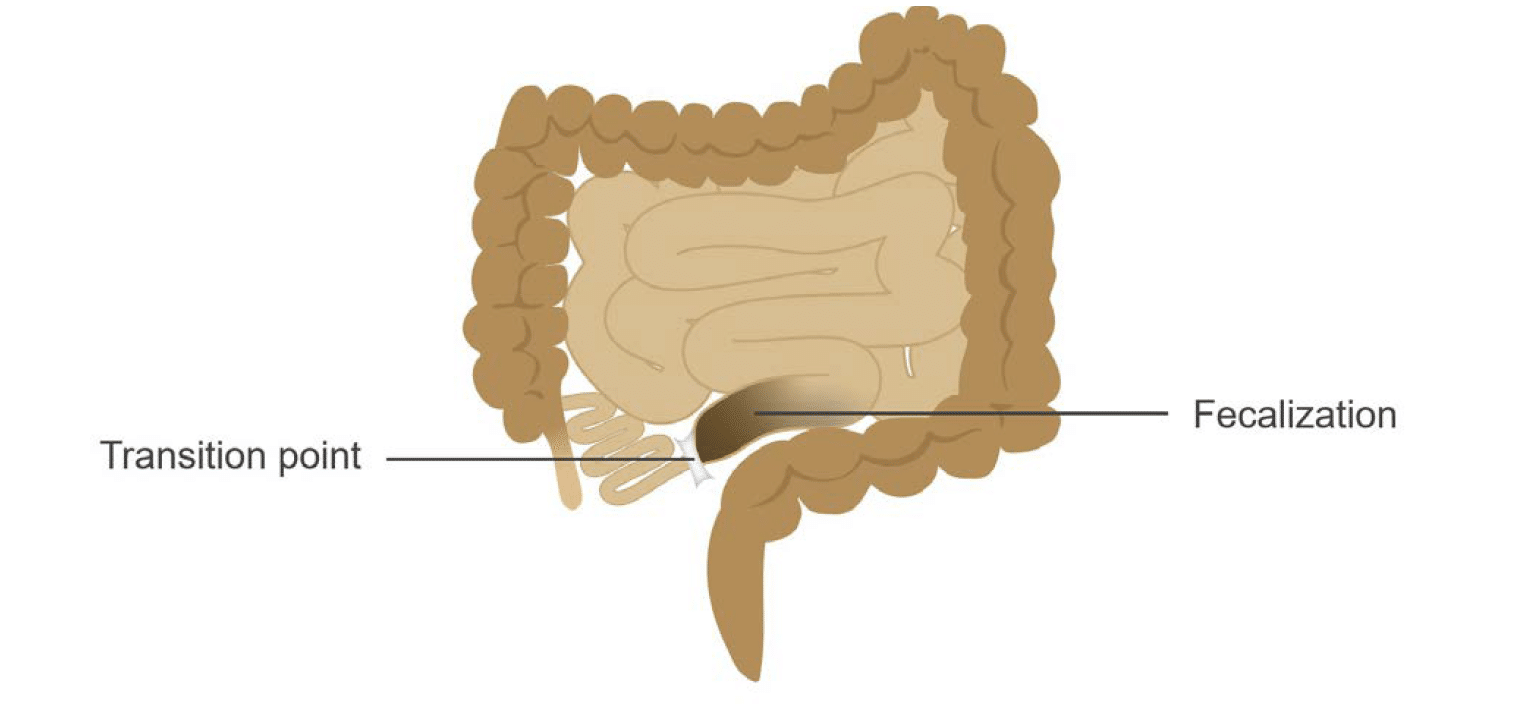
Transition point.
As you are following the dilated small bowel loops through the abdomen, look for tapering or angulation. This indicates the transition point where the small bowel changes from dilated, obstructed loops to normal, decompressed loops.
Identifying the transition point and carefully evaluating this area will help you determine the cause of the obstruction, whether it is adhesions or a more complex cause such as a mass, hernia, or a closed loop.
Faecalization.
This refers to the contents of the small bowel taking on the appearance of stool (i.e., faeces), which is characterized by little black dots of air. Normally, the contents of the small bowel are fluid-like, with faeces only arising in the colon.
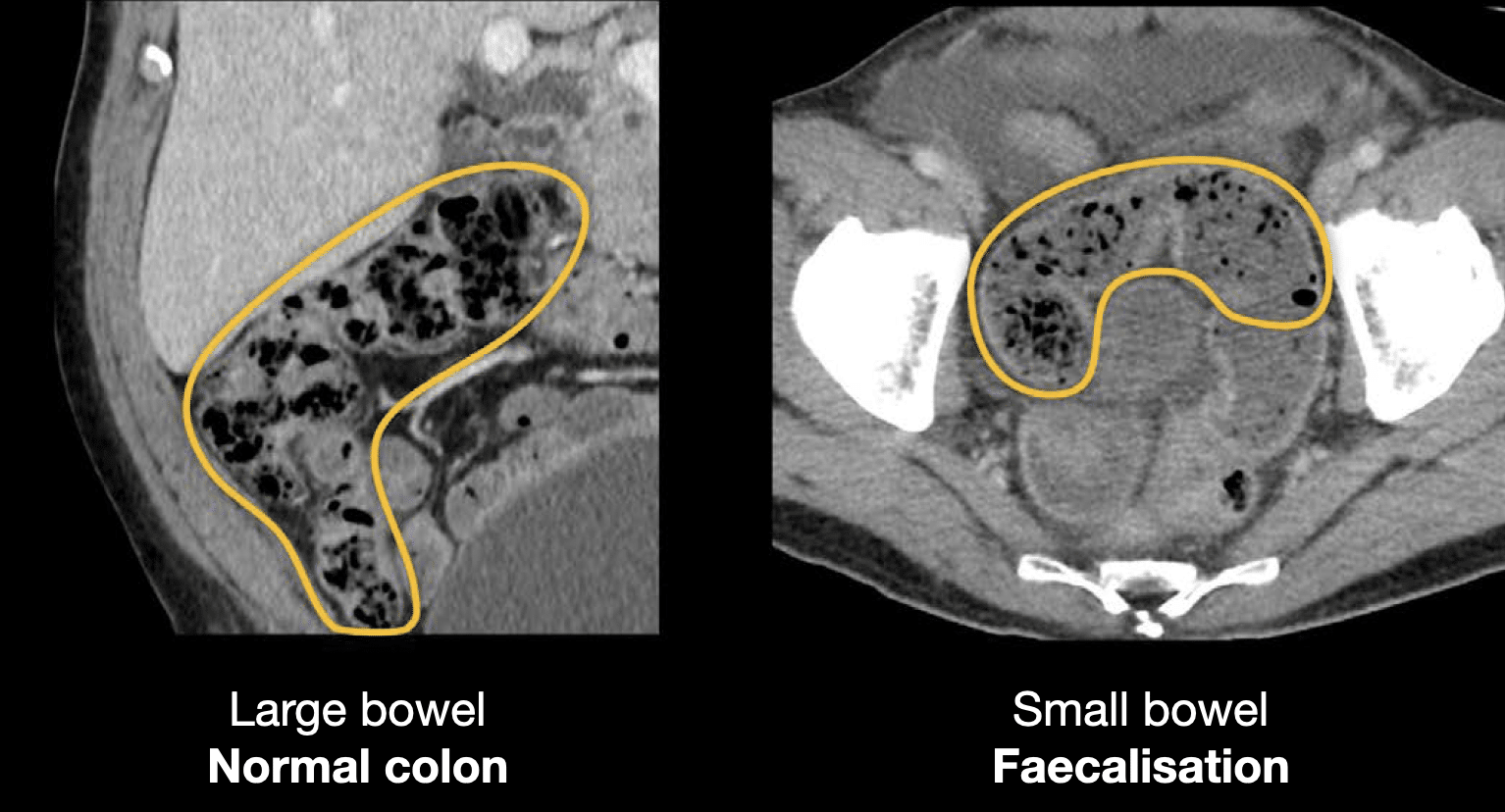
Faecalization normally occurs right before the transition point, and thus identifying it can help direct you to the cause of obstruction. Faecalization occurs because the bowel contents have remained stationary. Over time, the water content becomes resorbed, causing the contents to take on the appearance of stool.
Knowledge iteration
Let’s review a case to put our skills into practice. Scroll through the images provided in this online PACS clinical case
- Take a look at the distal oesophagus and stomach. You can see that the patient has oral contrast in these areas and that they are quite distended with food and contrast.
- Notice that the oral contrast does not make it very far before we quickly come to a transition where dilated loops of small bowel predominately contain fluid.
- Identify the transition point by noticing the faecalized loop of small bowel in the pelvis, which contains material similar to the ascending colon.
- Carefully follow this loop distally to find the tapering of the transition point, with distally decompressed small bowel leading to the terminal ileum.
This is an edited excerpt from the Medmastery course Abdominal CT Pathologies by Michael P. Hartung, MD. Acknowledgement and attribution to Medmastery for providing course transcripts
- Hartung MP. Abdominal CT: Common Pathologies. Medmastery
- Hartung MP. Abdominal CT: Essentials. Medmastery
- Hartung MP. Abdomen CT: Trauma. Medmastery
References
- Hartung MP. Abdominal CT: Imaging the small bowel
- Nickson C. Small bowel obstruction DDx. CCC
- Cadogan M. AXR Interpretation. CCC
- Nickson C. Abdominal X-ray and CT. CCC
- Top 100 CT scan quiz. LITFL
Radiology Library: Abdominal CT: Imaging important abdominal structures
- Hartung MP. Abdominal CT: acute appendicitis
- Hartung MP. Abdominal CT: diverticulitis
- Hartung MP. Abdominal CT: small bowel obstruction
- Hartung MP. Abdominal CT: closed loop small bowel obstruction
- Hartung MP. Abdominal CT: enteritis and colitis
- Hartung MP. Abdominal CT: peptic ulcer disease
- Hartung MP. Abdominal CT: peptic ulcer perforation
- Hartung MP. Abdominal CT: bowel perforation
Abdominal CT interpretation

Assistant Professor of Abdominal Imaging and Intervention at the University of Wisconsin Madison School of Medicine and Public Health. Interests include resident and medical student education, incorporating the latest technology for teaching radiology. I am also active as a volunteer teleradiologist for hospitals in Peru and Kenya. | Medmastery | Radiopaedia | Website | Twitter | LinkedIn | Scopus

MBChB (hons), BMedSci - University of Edinburgh. Living the good life in emergency medicine down under. Interested in medical imaging and physiology. Love hiking, cycling and the great outdoors.