
![]()
Colles fracture
Description
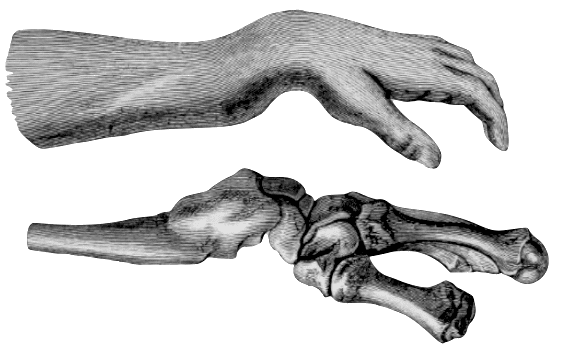
Colles fracture: Extra-articular fracture of the distal radius with dorsal angulation of the distal fragment. Frequently associated with an ulna styloid fracture and volar angulation of the fracture apex

History of the Colles fracture
Hippocrates described traumatic injuries about the wrist as dislocations. He defined four distinct directions of dislocations, and his influence extended for nearly 2000 years through the writings of Gallen, Palladius, Celsus, Duverney, and Fabricius.
The joint of the hand is dislocated either inward or outward, most frequently inward.
1705 – Early in the eighteenth century, French surgeon Jean-Louis Petit suggested that traumatic swelling and displacement at the wrist was as a result of a distal radius fracture rather than a luxation or dislocation as previously believed.
Original
English
“A l’égard du déplacement selon sa longueur, je sçais que l’on peut le disputer dans la fracture d’un seul os: mais nous le prouverons ci-après d’une maniere à n’en pas douter”
Petit JL. De la fracture de l’avant bras 1705; 2: 115-126
“As to the displacing length-ways, I know it may be disputed in the fracture of one bone only: But I shall prove it hereafter so as to leave no Room to doubt it.”
Petit JL. De la fracture de l’avant bras 1705; 2: 115-126
1760 – Claude Pouteau recognized the lesion at the wrist as a fracture, rather than a dislocation, of the distal end of the radius with dorsal angulation of the distal fragment
Original
Tab Title
“…mais il sera question principalement des fractures qui arrivent après des chûtes, ou la main paroit avoir fait les plus grands efforts pour en parer le danger. Ces fractures sont le plus souvent prises pour des entorses, pour des luxations incomplettes…
Il n’est peut-être point de fracture plus facile à reconnoitre au simple coup d’oeil, que celles du radius ou du cubitus, près du poignet… ses signes sont très remarquables; la moindre largeur de l’avant bras au centre de la fracture, sa dépression contre nature, par la saillie de l’une ou l’autre apophyse styloïde, & une plus grande largeur du poignet.
…lorsque le radius est cassé, sa partie inférieure est toute livrée à la force pronatrice du plan supérieur du muscle quarré”
Pouteau C, 1783;2:251-253
“…but we shall concern ourselves principally with fractures that occur following falls, where the hand appears to have made the greatest efforts to stave off danger. These fractures are most often taken for sprains, for incompete luxations…
There is hardly any fracture easier to recognize at a simple glance, than that of the radius or the ulna near the wrist… its signs are very remarkable; the reduced width of the forearm at the centre of the fracture, its unnatural depression, by the protrusion of the one or other styloid apophysis, & a larger width of the wrist
…when the radius is broken, its inferior part succumbs to the pronating force from the superior plane of the pronator quadratus muscle”
Pouteau C, 1783;2:251-253
1795 – Pierre-Joseph Desault alluded to the combination of a fracture and dislocation but did little to shed light on distinguishing between the two or to suggest any alteration in treatment.
Original
English
“Il est une circonstance dependant, où voisine de l’articulation du carpe, la division peut donner à des apparences qui mentent une luxation de cette partie. Alors en effet, comme dans celle-ci, quelquefois une convexité en arrière, une dépression en devant, ou réciproquement se font àppercevoir; effet du déplacement des fragment.”
“There is a circumstance, however, where a fracture near to the joint of the wrist, may give rise to appearances similar to a luxation of that part. In both cases, indeed, a convexity behind, and a depression before, or the reverse, are perceived, and are the effect of a displacement of the fragments.”
1814 – Abraham Colles provided a description of the symptoms of a fracture of the carpal extremity of the radius in the time before X-ray. Aware his comments would cause intense debate and conjecture, he made certain to assuage his contemporaries with regard to the likely reasons for previous confusion…
The injury to which I wish to direct the attention of surgeons has not, as far as I know, been described by any author; indeed the form of the carpal extremity of the radius would rather incline us to question its being liable to fracture. The absence of crepitus and of the other common symptoms of fracture, together with the swelling which instantly arises in this, as in most other injuries of the wrist, render the difficulty of ascertaining the real nature of the case very considerable.
Colles contradicted previous belief that these injuries were dislocations of the carpus from the wrist.
This fracture takes place at about an inch and a half * above the carpal extremity of the radius, and exhibits the following appearances. The posterior surface of the limb presents a considerable deformity; for a depression is seen in the fore-arm, about an inch and a half above the end of this bone, while a considerable swelling occupies the wrist and metacarpus. Indeed, the carpus and base of metarcarpus appear to be thrown backward so much, as on first view to excite a suspicion that the carpus has been dislocated forward.
Colles, 1814:183
Colles described a means of examination to confirm the distal radius fracture.
I hit upon the following simple method of examination, by which I was enabled to ascertain that the symptoms above enumerated actually arose from a fracture seated about an inch and a half above the carpal extremity of the radius. Let the surgeon apply the fingers of one hand to the seat of the suspected fracture, and, locking the other hand in that of the patient, make a moderate extension, until he observes the limb restored to its natural form; so soon as this is effected, let him move the patient’s hand backward and forward, and he will, at every such attempt, be sensible of a yielding of the fractured ends of the bone, and this to such a degree as must remove all doubt from his mind
…and further emphasised the clinical features to distinguish distal radius fracture from luxation.
The nature of the injury once ascertained, it will be a very easy matter to explain the phenomena attendant on it, and to point out a method of treatment which will prove completely successful. The hard swelling which appears on the back of the hand is caused by the carpal surface of the radius being directed slightly backwards, instead of looking directly downwards.** The carpus and metacarpus, retaining their connexions with this bone, must follow it in its derangements, and cause the convexity above alluded to.
In contrast to Petit and Pouteau, Colles was confident in his observations, even without post mortem evidence. His conclusions were firm and direct, and left no doubt that he had described a fracture and not a dislocation.
I should consider this as by far the most common injury to which the wrist or carpal extremity of the radius and ulna are exposed. During the last three years I have not met with a single instance of Desault’s dislocation of the inferior end of the radius, while I have had opportunities of seeing a vast number of the fractures of the lower end of this bone.
Colles, 1814
1847 – Smith bestowed eponymous immortality upon Colles. He recounted Colles’ description in full, adding sketches and further defining the clinical presentation and course
The fracture is usually the result of a fall upon the palm of the hand, and is liable to happen whenever a person, in the act of falling forwards, throws out before him his arms and hands in a state of extension, which he does, as it were, instinctively, to save the head and face from injury.
Smith 1847;140
Smith refined the Colles’ anatomical description with corrections footnotes:
- (*)The situation of the fracture is not so high as Mr. Colles states it to be; I have never seen it more than an inch above the carpal end of the bone
- (**) The carpal surface of the radius does not look directly downwards, its aspect is downwards, forwards, and very slightly inwards
He acknowledged the work of Petit and Pouteau work but believed Colles name should be related to the fracture. Smith even referred to Pouteau’s original description in his defining of the Colles fracture…
…there is no fracture the existence of which it is more easy to tell at a single “coup d’oeil“
Smith 1847;140
1897 – With the advent of X-Ray (Röntgen-rays) the knowledge of fractures, dislocations and their management grew dramatically. Carl Beck (1856–1911) professor of surgery at the New York Post-Graduate School of Medicine observed 44 cases of ‘Colles fracture’, 1896-1897 with X-Ray (skiagram).

It may be safely said that treatises on this subject which were written before the Röntgen era have ceased to be regarded as authoritative. Following the new discovery great interest was at once concentrated on the much disputed classic fracture of the lower end of the radius, and it soon became evident that a much greater variety of the different types of this fracture (which represents ten per cent, of all fractures) exists than was ever anticipated before.
Most of the skiagrams revealed conditions not thoroughly anticipated when examined by the usual methods. One most surprising feature was that in nineteen of these cases a distinct transverse fissure above the capitulum ulnae existed, without causing any apparent symptoms. In seven cases the styloid process of the ulna was entirely broken off.
Prof Carl Beck 1898
1900 – The American surgeon Ernest Amory Codman (1869 – 1940) further classified the distal radius fractures following the introduction and x-rays and ‘skiagrams’. He divided distal radius fractures into ten (X) Classes. The ‘typical Colles fracture – Class VIII‘ occurred in 46% of the 140 x-rays examined
Codman Classification

- Class I (Base styloid process of radius);
- Class II (Inner angle of distal radius);
- Class III (Transverse fracture distal to epiphyseal line);
- Class IV (Salter-Harris III);
- Class V (Salter-Harris I);
- Class VI (Salter-Harris II);
- Class VII (Salter-Harris V);
- Class VIII (typical Colles fracture);
- Class IX (stellate fracture with longitudinal fissures);
- Class X (‘reversed Colles fracture’ though looks more like a Barton fracture than a Smith fracture…)
Associated Persons
- Jean-Louis Petit (1674–1750)
- Claude Pouteau (1724–1775)
- Jean-Gaspard Blaise Goyrand (1803-1866) [Goyrand fracture]
- Pierre-Joseph Desault (1738 – 1795)
- Abraham Colles (1773 – 1843) [Colles fracture]
- Robert William Smith (1807-1873) Re-evaluation and naming of Colles fracture
- Edward Mott Moore (1814-1902) [Moore fracture]
- Carl Beck (1856–1911) Early radiographs of Colles fracture
- Ernest Amory Codman (1869–1940) Codman Classification
Alternative names
- Pouteau fracture (commonly used in France).
- Dinner fork deformity; bayonet deformity
References
Historical references
- Petit JL. De la fracture de l’avant bras. In: L’art de guérir les maladies des os, 1705; 2: 115-126 [Translation: Of the fracture of the Fore-Arm. In: A treatise of the diseases of the bones, 1726; 2(XI): 287-295]
- Pouteau C. Memoire, contenant quelques reflexions sur quelques fractures de l’avant-bras sur les luxations incomplette du poignet sur les diastasis. In: Oeuvres Posthumes de M Pouteau. Paris. 1783;2:251-266 [Pouteau-Colles fracture]
- Colles A. On the fracture of the carpal extremity of the radius. The Edinburgh medical and surgical journal. 1814;10:182-186.
- Smith RW. On Fractures of the Bones of the Fore-arm in the Vicinity of the Wrist Joint. In: A Treatise on Fractures in the Vicinity of Joint and on Certain Forms of Accidental and Congenital Dislocations. 1847: 129-175
- Beck C. Colles’ fracture and the roentgen rays. Medical News 1898; Feb: 230-232
- Codman EA. A Study of the X-Ray Plates of One Hundred and Forty Cases of Fracture of the Lower End of the Radius. The Boston Medical and Surgical Journal. 1900;143(13): 305-308.
Review references
- Peltier LF. Eponymic fractures: Abraham Colles and Colles’ fracture. Surgery. 1954 Feb;35(2):322-8
- Peltier LF. Six eponymic fractures. Bull Med Libr Assoc. 1960 Jul;48(3):345-51.
- Fernandez DL, Jupiter JB. Fracture of the Distal End of the Radius: Historical Perspective. In: Fractures of the Distal Radius. 2002: 1-21
eponymictionary
the names behind the name

Dr Ronan McKenna, MB BCh BAO at National University of Ireland Galway. Living in Australia with plans for a future in Emergency Medicine. A keen interest in Medical History, Wilderness Medicine and Sport.
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |
