
![]()
ECG Case 043
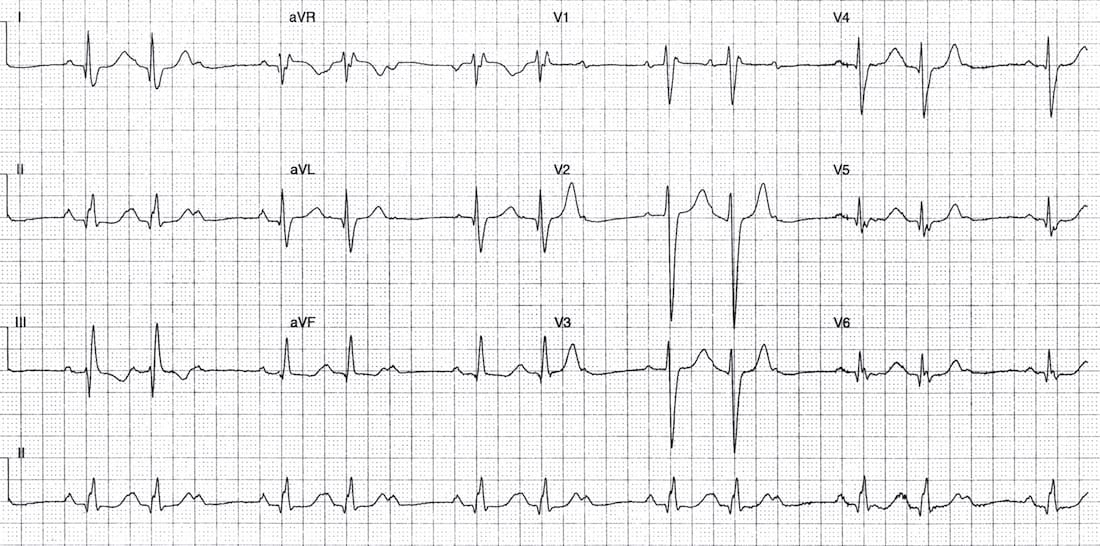
Middle-aged patient presenting with syncope. Describe the ECG
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
Main Abnormalities
Sinus rhythm with evidence of 2nd degree AV block
- The QRS complexes cluster in groups separated by non-conducted P waves.
- There is a 3:2 relationship between the P waves and QRS complexes.
- With fixed ratio blocks like this, it can sometimes be difficult to distinguish between Mobitz I and Mobitz II conduction, as there are not always enough successive PR intervals to judge whether progressive PR prolongation is occurring.
- The PR interval seems relatively constant between the first and second beats of each group, suggesting Mobitz II conduction.
- However, the clustering of QRS complexes into repeating groups with P:QRS ratios of 3:2, 4:3, 5:4, etc. is a characteristic feature of Mobitz I.
- There is an atypical RBBB — typical RSR’ pattern in V1 with slurred S wave in lead I, but atypical morphology elsewhere.
Pragmatically, I wouldn’t get too focussed on trying to work out the rhythm from a single tracing. I would just record multiple ECGs aiming to capture any longer P:QRS cycles to assess whether successive PR prolongation is present (Mobitz I) or absent (Mobitz II).
Progressive PR prolongation with Mobitz I

Constant PR interval with Mobitz II

Another clue to aid differentiation is QRS width:
- Mobitz I is typically due to block at the level of the AV node — hence QRS complexes are usually (but not always) narrow.
- Mobitz II typically occurs on a background of widespread conducting system disease (LBBB or bifascicular block). The block is typically at the level of the fascicles — hence QRS complexes are usually (but not always) broad.
CLINICAL PEARLS
There is some prognostic value in differentiating between Mobitz I and II — Patients with Mobitz II have a much higher rate of complete heart block and are more likely to require a permanent pacemaker.
However, in the acute situation it is more important to look at the patient rather than to fixate on the ECG.
Treatment decisions such as whether to commence temporary pacing will be largely determined by the patient’s clinical stability.
FURTHER READING
Related Topics
- AV block: 1st degree
- AV block: 2nd degree, Mobitz II
- AV block: 2nd degree, “fixed ratio blocks” (2:1, 3:1)
- AV block: 2nd degree, “high grade AV block”
- AV block: 3rd degree (complete heart block)
- Eponymythology: History of Second-degree AV block. LITFL
- Eponym: Karel Frederik Wenckebach (1864-1940). LITFL
- Eponym: Woldemar Mobitz (1889-1951). LITFL
- Eponym: John Hay (1873-1959). LITFL
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
TOP 100 ECG Series
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |