![]()
ECG Case 135
16-year-old female with intentional polypharmacy overdose. HR 72 reg, BP 100/62, GCS 15.
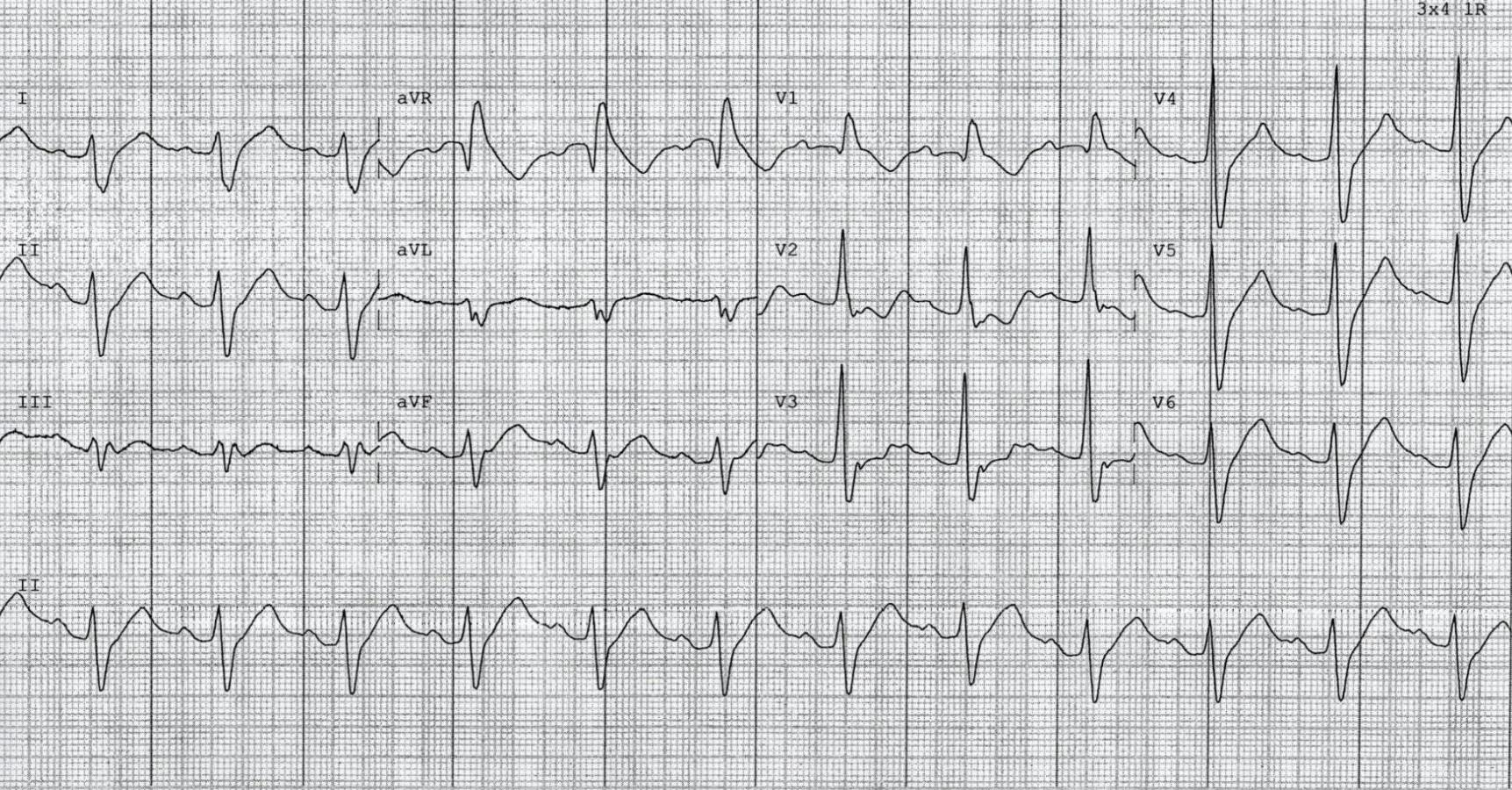
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
- Sinus rhythm, rate 72 bpm
- 1st degree AV block (PR interval ~210ms)
- Northwest axis
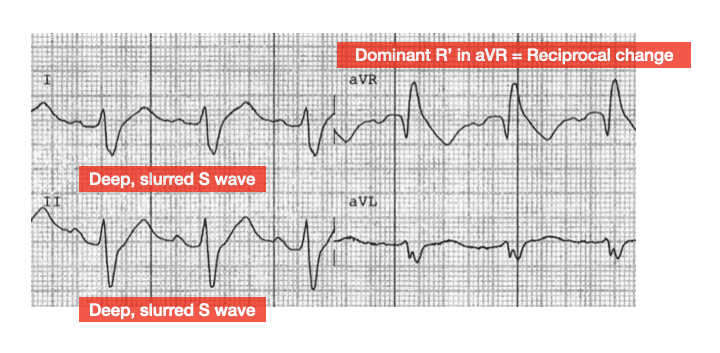
- Dominant R’ wave in aVR reflects terminal right axis deviation of the QRS
- There is marked intraventricular conduction delay (IVCD) with QRS duration ~160ms
- Absolute QT interval is 460ms
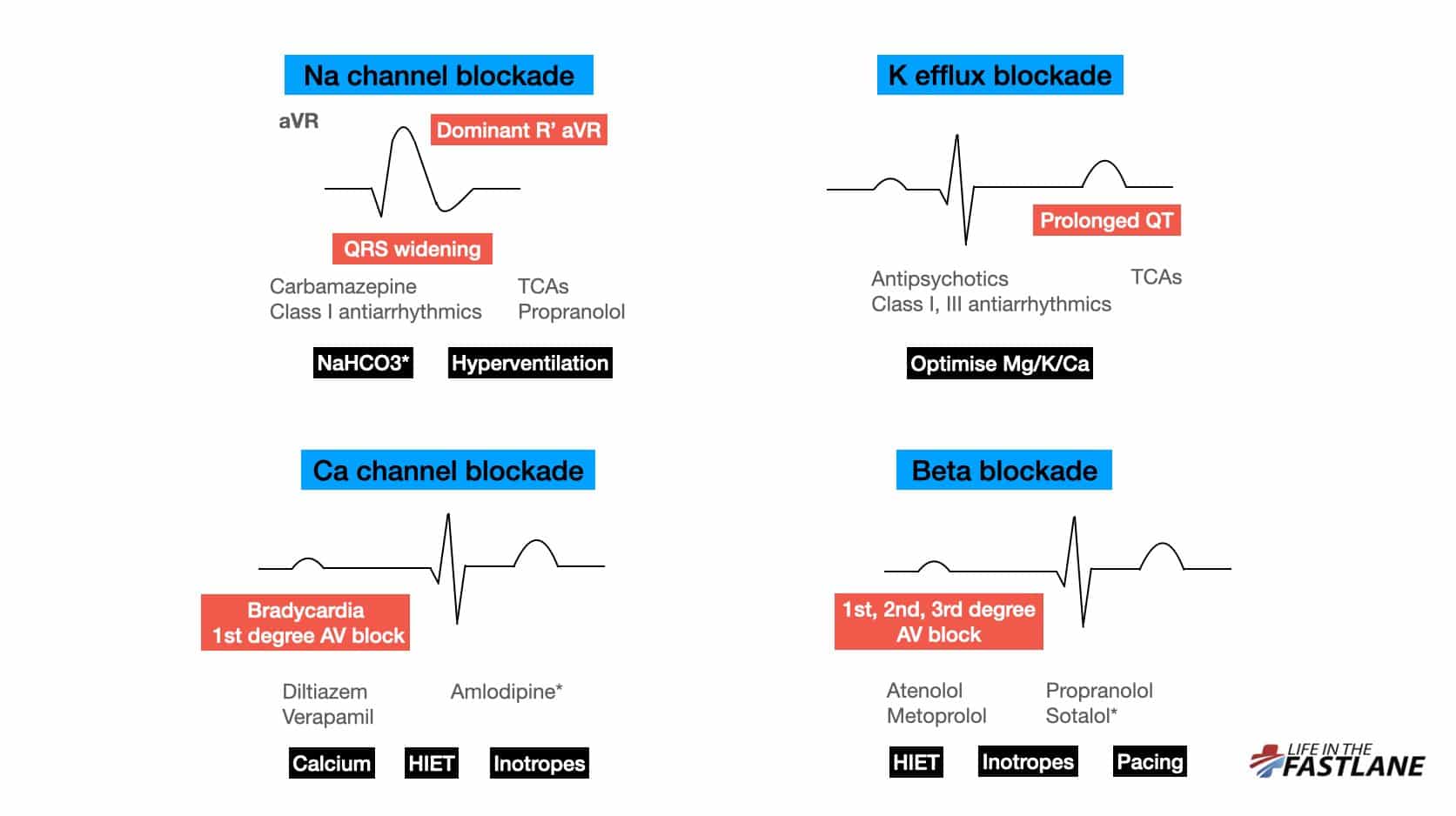
This patient has three important toxicological ECG manifestations — there are features of AV blockade, sodium channel blockade, and potassium efflux blockade.
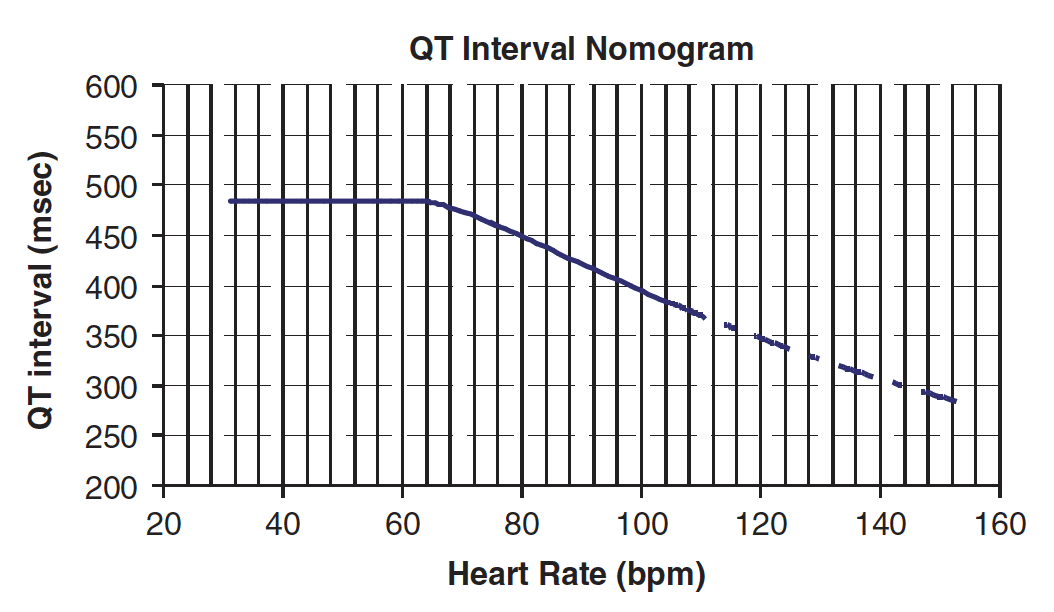
Such marked QRS widening places them at risk of both seizures and ventricular arrhythmias. An absolute QT interval of 460ms is on the borderline of the tox nomogram — this patient is likely at risk of Torsades de Pointes (TdP).
OUTCOME
This patient had ingested 2500mg of immediate release flecainide. They were commenced on a bicarbonate infusion titrated to reduce IVCD and associated risk of seizures/ventricular arrhythmias. Inotropes were not required and the patient made an uneventful recovery.
CLINICAL PEARLS
Understanding ECG changes makes them easier to recognise
We may have heard that Na channel blockade causes “right axis deviation of the terminal QRS”. But what does this actually mean?
Well, the right-sided intraventricular conduction system is more susceptible to Na channel blocker toxicity than the left. This leads to delayed depolarisation of the right ventricle (RV). As is the case in right bundle branch block (RBBB), delayed RV conduction manifests as deep, slurred S waves in leads I, II, V5-6.
aVR is not a real lead – it is calculated from leads I and II and is a mirror (reciprocal) image of changes seen in these leads:
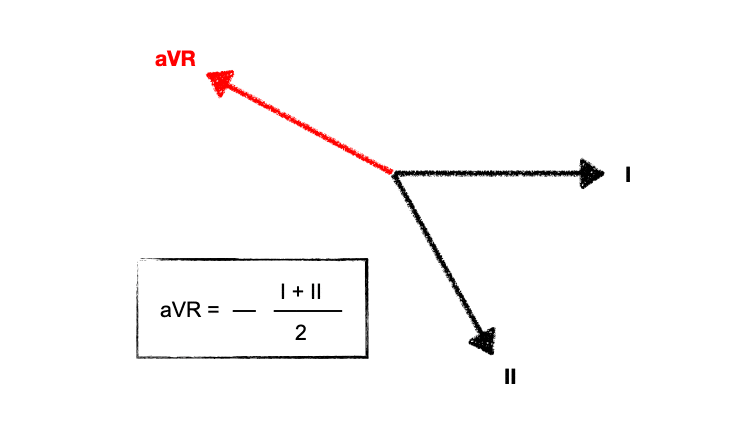
Deep, slurred S waves of delayed RV conduction are thus reflected as a dominant R’ wave in aVR. The “amplitude” of R’ in aVR is mentioned frequently, but actually the pattern recognition of a widened R wave is just as important.
With worsening toxicity, left-sided conduction pathways are increasingly affected, eventually leading to a “sine wave” appearance reminiscent of hyperkalaemia.
Patients with tricyclic antidepressant (TCA) overdose are at increased risk of seizures with QRS > 100ms, and of ventricular dysrhythmias with QRS > 160ms. In practice, we assume this holds true for all types of sodium channel blockade, however the risk likely varies with differing agents. A cut-off of 200ms may be more relevant for flecainide overdose (see below).
NaHCO3 can improve conduction delay with resultant shortening of QRS. However, there can be a variable response to this. Do not continue to give repeated boluses unless there is a clear response. There have been case reports of death from this.
How and where do we measure the QT interval?
A reminder on measuring the QT interval. Don’t rely on the computer. The biggest pitfall of computer interpretation is including separate U waves in calculations, which leads to falsely high measurements of 600ms+.
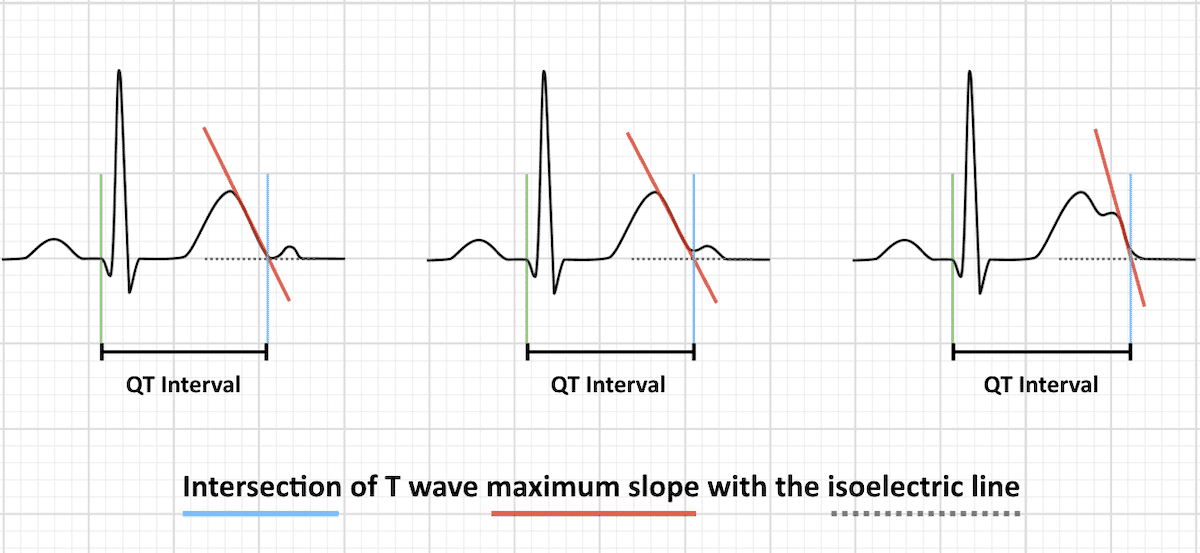
There is no specific correct lead to measure – simply use the lead with the longest interval. The general recommendation to measure II or V5-6 comes from the fact that these leads usually correlate to the overall vector of depolarisation.
In tox ECGs, the absolute value can measured and plotted on the nomogram to predict if patients are at risk of TdP (Torsades de Pointes). Use this as opposed to QTc.
Read more about the effects of beta blocker and calcium channel blocker overdose on the ECG here.
Flecainide in overdose
Flecainide is a class IC anti-arrhythmic that exerts its action through potent blockade of Na and K channels with slow unblocking kinetics. At normal doses it does not prolong the action potential duration or QT interval.
Toxic dose is not well-established but is seen with ingestion as low as five times usual daily dose.
Its effects at therapeutic levels are greatest on the His-Purkinje system and ventricular myocardium, but with increasing toxicity extend to the AV node and atria and also cause left ventricular (LV) dysfunction.
Flecainide overdose appears to present with one of two morphologically distinct patterns based on the QRS duration. Patients with QRS duration < 200ms are likely to demonstrate a RBBB pattern, visible P waves, and relatively shorter QT interval. Those with QRS > 200ms are more likely to show LBBB, loss of P waves, a northwest axis, and a longer QT interval. Deaths have only been reported in patients with QRS duration > 200ms.
In therapeutic doses flecainide can be used for diagnostic purposes in patients with type 2 or 3 Brugada ECG patterns. However, in large ingestions patients without this congenital abnormality may also manifest an ECG resembling Brugada Syndrome.
The role of alkalinisation is less established than in other forms of Na channel blocker toxicity — NaHCO3 is indicated for patients with QRS prolongation or hypotension, but patients who do not respond to initial doses are unlikely to benefit from further administration. Inotropes may be required to support hypotension — ideally the choice of agent should be guided by bedside echo findings.
- ECG manifestations of Na channel blocker toxicity are primarily due to effects on the right-sided intraventricular conduction system — look for a widened QRS complex and a dominant, broad R’ wave in aVR
- Always measure the QT interval yourself. There is no specific correct lead to measure — simply use the lead with the longest interval
- Flecainide overdose appears to present with one of two morphologically distinct ECG patterns depending on QRS duration (< or > 200ms)
Further reading
Related topics
- Buttner R. Pharm 101: Flecainide
- Burns E, Buttner R. ECG features of sodium channel blockade
- Nickson C. ECG in Toxicology
Expert Review
- Smith SW. Agitation and tachycardia – sodium channel blockade Dr Smith’s ECG Blog. 2014 May
References
- Murray et al. Toxicology Handbook 3e. Elsevier Publishing. 2015 February
- Valentino et al. Flecainide toxicity: A Case Report and Systematic Review of its Electrocardiographic Patterns and Management. Cardiovasc Toxicol. 2016 Jul
- Ghataoura et al. Flecainide toxicity: a presentation to the emergency department with literature review. BMJ Case Report. 2020 Feb
Further reading
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
TOP 150 ECG Series

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC

Interventional cardiologist, ECG and hemodynamics fan. MD, Assoc. Prof. at Marmara University, Pendik T&R Hospital, Assoc. Editor at Archives of TSC, ESC National Prevention Coordinator