
![]()
History of epidural needles and catheters
Epidural needles are hollow needles used to locate the epidural space without intentionally puncturing the dura. Unlike spinal needles, which confirm subarachnoid placement by free flow of cerebrospinal fluid, epidural needles rely on indirect signs of position such as tactile feel, loss of resistance, the hanging-drop sign, controlled injection, and later catheter passage.
The epidural needle must cross skin, ligament and ligamentum flavum reliably, stop short of the dural sac, and permit injection or catheter placement. Additionally they must minimise the risk of accidental dural puncture, vascular cannulation, catheter kinking, catheter shearing, unilateral block and failed analgesia.
The history of epidural anaesthesia begins with caudal access to the sacral epidural space, moves through lumbar and thoracolumbar localisation, and then covers continuous techniques. Once clinicians wanted to leave a catheter in the epidural space the needle-tip geometry, bevel direction, hub design, stylet fit, catheter material, catheter stiffness and orifice arrangement became central. The “Tuohy needle” became the dominant generic term, but its lineage is more complex.
Design variables in epidural needles and catheters
Needle tip / bevel: Epidural needle bevels influence tactile feel, passage through ligamentum flavum, dural indentation, likelihood of dural puncture, and the direction in which a catheter exits the needle.
Curved or directional tip: The Huber–Tuohy concept directed a catheter as it emerged from the needle. This became central to continuous epidural catheter placement.
Orifice and heel: The size, shape and position of the needle opening affect catheter passage. Later refinements, especially Hustead-type designs, attempted to reduce catheter trapping or shearing at the heel of the needle.
Hub and wings: Hub design affects control during slow advancement. Weiss-style wings improved two-handed handling, particularly for hanging-drop localisation.
Stylet / obturator: Stylets reduce tissue coring and obstruction. Poorly matched or protruding stylets, however, could create new problems, as seen with the Tuohy–Flowers modification.
Catheter material: Early continuous techniques adapted silk or nylon ureteral catheters. Later plastic catheters improved sterility, cost, handling, kink resistance and reliability.
Catheter tip and orifices: Modern catheter design shifted attention to material stiffness, open- or closed-tip configuration, and single- versus multi-orifice designs, all of which may influence spread, paraesthesia, intravascular placement, migration, kinking, breakage and removal.
Chronology of epidural needles and catheters
Caudal access and early sacral extradural anaesthesia
1901 – Caudal epidural access. Jean-Anthanase Sicard (1872–1929), French neurologist, and Fernand Cathelin (1873–1960), French physician and urologist, independently introduced sacral/caudal epidural injection through the sacral canal. Sicard emphasised sacrococcygeal extra-dural medication whilst Cathelin described the sacral canal route, animal validation, and early human applications. [Sicard 1901; Cathelin 1901]
1909–1910 – German sacral anaesthesia. Walter Stoeckel (1871–1961), German gynaecologist, adapted caudal epidural injection for obstetric analgesia and helped establish the term sacral anaesthesia. Arthur Georg Läwen (1876–1958), German surgeon, extended the method into operative regional anaesthesia using larger-volume alkalinised, suprarenin-containing novocaine and later the term extradural anaesthesia. [Stoekel 1909; Läwen 1910]
1917 – Upper sacral extradural anaesthesia. Salvador Gil Vernet (1892–1987), Spanish urologist and anatomist, described an anatomy-led sacral extradural technique for prostatic surgery. His lateral sacral canal approach aimed to achieve higher pelvic and lower lumbar blockade without dural puncture.
Lumbar epidural localisation
1921 – Thoracolumbar epidural anaesthesia. Fidel Pagés Miravé (1886–1923), Spanish militarysurgeon, described single-shot thoracolumbar epidural anaesthesia as anestesia metamérica, a segmental surgical block produced outside the dura. His early death and publication in Spanish military literature limited dissemination, and the technique was later rediscovered and popularised through Dogliotti’s work.
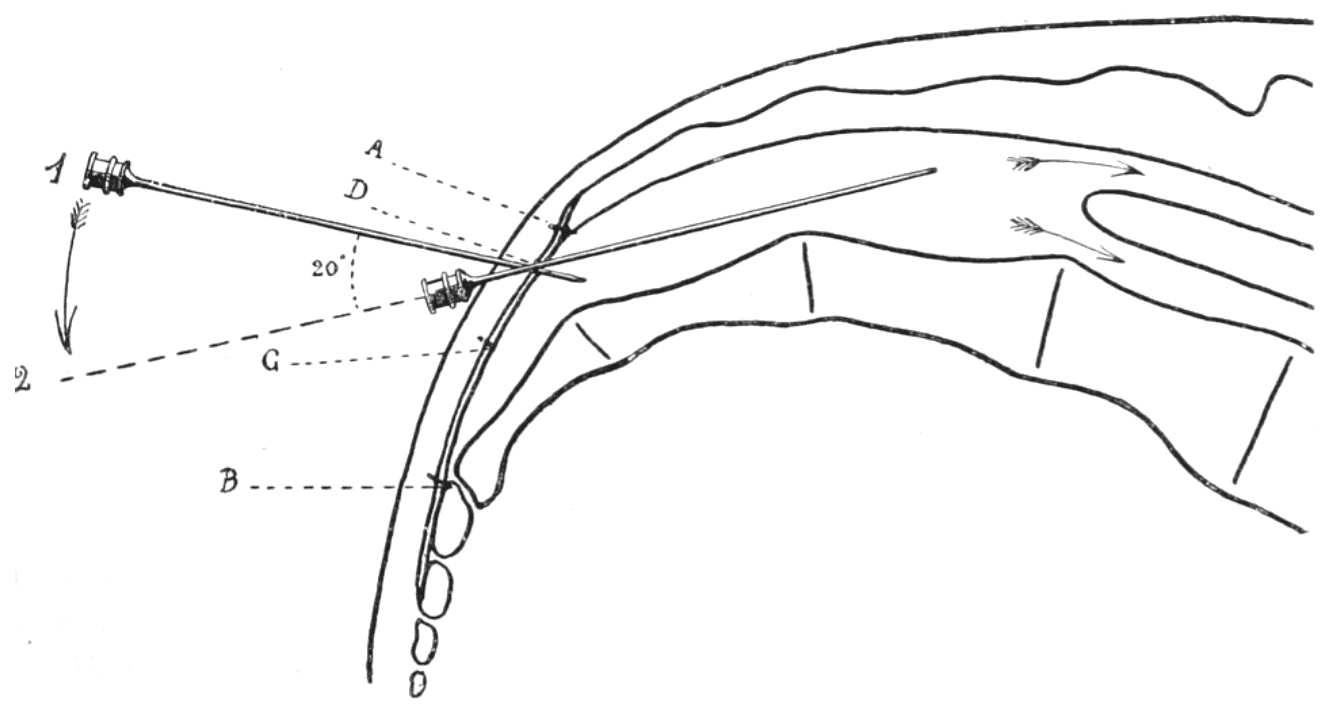
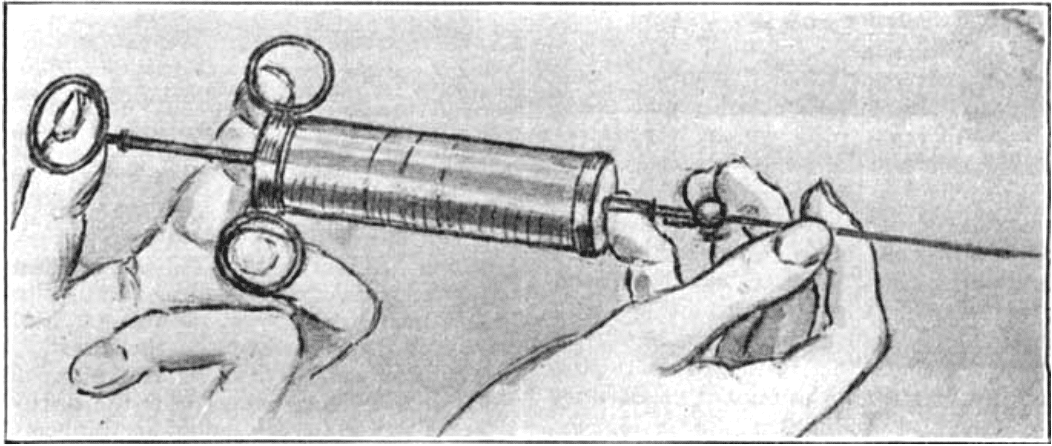
1931–1933 – Loss of resistance. Achille Mario Dogliotti (1897–1966), Italian surgeon, popularised lumbar peridural anaesthesia and described the practical loss-of-resistance method for identifying the epidural space. With steady pressure on a saline-filled syringe, resistance suddenly disappeared as the needle passed the ligamentum flavum into the epidural space.
1932 – Visual epidural aspiration. Angelo Luigi Soresi (1877-1951), Italian-American surgeon, published an early peridural anaesthesia report that deserves a priority note. Soresi should be recognised for the first published observation of negative-pressure epidural space localisation.
I call the attention of the reader to a phenomenon which, to my knowledge, has not been described…The surgeon watches carefully the fluid in the shank of the needle while pushing very slowly the needle toward the spine. Suddenly it will be noticed that the fluid disappears from the shank, as if it had been sucked away. This phenomenon indicates that the needle has entered the epidural space.
Soresi 1932
1933 – The hanging drop. Alberto Gutiérrez (1892–1945), Argentine surgeon, described the gota colgante or hanging-drop sign as a practical visual method for epidural localisation. A droplet placed at the needle hub was drawn inward when the needle entered the epidural space.
Continuous techniques create a hardware problem
1931–1938 – Continuous obstetric epidural concepts. Eugen Bogdan Aburel (1899-1975, Romanian obstetrician-gynaecologist, described one of the earliest catheter-through-needle techniques for continuous labour analgesia. He introduced a soft silk catheter through a caudal or lumbar needle, withdrew the needle, and left the catheter in situ for repeated injections of local anaesthetic during labour. Aburel deserves recognition for both his lumbosacral approach and his early concept of continuous peridural analgesia. [Aburel 1931]
1940 – Continuous spinal hardware. William Thomas Lemmon (1896–1974), American surgeon, developed continuous spinal anaesthesia using a malleable spinal needle left in the lumbar subarachnoid space, connected to tubing and stopcocks for repeated fractional dosing. Although intrathecal rather than epidural, Lemmon’s system highlighted the hardware problem. Continuous neuraxial anaesthesia required secure fixation, durable needles, sterile tubing, reliable flow, and patient positioning that did not kink or dislodge the apparatus. [Lemmon 1940]
1942 – Continuous caudal analgesia. Robert Andrew Hingson (1913–1996), American anaesthesiologist, and Waldo B. Edwards (1905–1981), American obstetrician, adapted the continuous concept to the caudal epidural route for labour and delivery. Their malleable caudal needle could follow the curve of the sacral canal and remain in place for prolonged fractional dosing, converting caudal block from an intermittent injection into titratable obstetric analgesia. [Edwards 1942]
1942-1943 – Continuous caudal reports. Samuel A. Manalan (1912–1990) reported caudal block anaesthesia in obstetrics, representing the wider American uptake of caudal obstetric analgesia. At Mayo Clinic, R. Charles Adams, John Silas Lundy (1894–1973), and Thomas H. Seldon (1905–1991) reported continuous caudal anaesthesia/analgesia, discussing technique, uses, and possible dangers. [Manalan 1942; Adams 1943]
1943 – Southworth, Hingson and the failed lumbar transition. James L. Southworth and Hingson extended continuous caudal analgesia into surgical practice and then attempted a lumbar continuous epidural approach. They used a large Barker spinal needle and silk ureteral catheter, but the system was technically difficult, with only partial success. Maintaining catheter position through a sharp lumbar needle was too unreliable, and later directional needle systems were needed. [Southworth 1943]
The most important part of the apparatus is the malleable needle… constructed so that it will assume the curvature of the sacral canal for many hours under considerable stress without breakage and without obliteration of the lumen… In our series it has been used more than four hundred times without breakage.
Hingson, Edwards 1943
Directional needle era
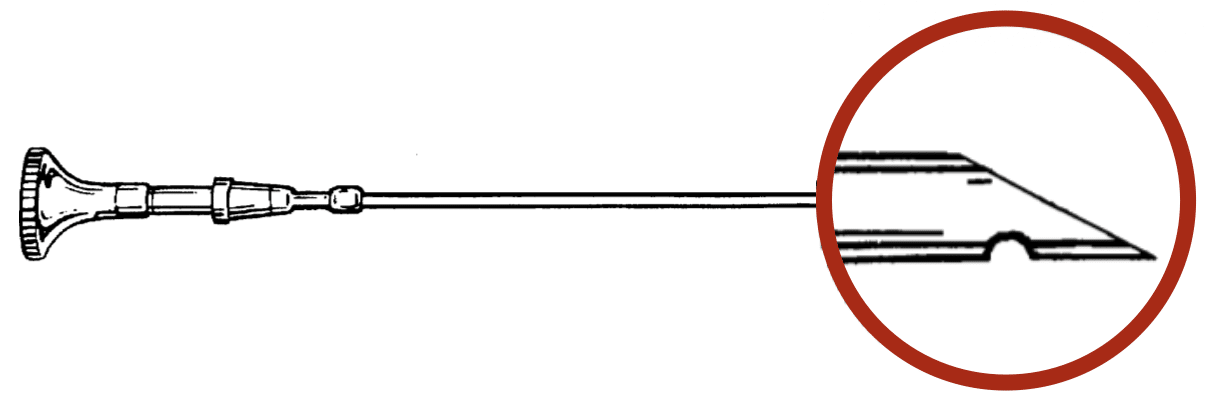
1944–1946 – Ralph L. Huber (1889–1953), Seattle dentist and inventor, developed a curved, non-coring hypodermic needle with a lateral opening, patented in 1946. Edward Boyce Tuohy (1908–1959), American anaesthesiologist, recognised that this directional Huber-type point could facilitate neuraxial catheter passage and adopted it for continuous spinal anaesthesia, adding a stylet and popularising the device in anaesthetic practice as the “Tuohy needle.”
1947–1949 – Continuous lumbar epidural catheterisation. Manuel Martínez Curbelo (1906–1962), Cuban anaesthesiologist, adapted Tuohy’s continuous spinal catheter method to the epidural space after observing Tuohy at the Mayo Clinic in 1946. On January 13, 1947, he threaded a No. 3.5 ureteral catheter through a 16-gauge Tuohy needle with Huber point into the lumbar peridural space. He presented the method in 1947 and published it in 1949.
1949 – Charles E. Flowers Jr (1920–1999), Louis M. Hellman (1908–1990), and Hingson applied continuous peridural anaesthesia and analgesia to labour, delivery and caesarean section. Their key practical modification was the use of plastic tubing rather than a ureteral catheter, threaded through a 16-gauge Tuohy needle.
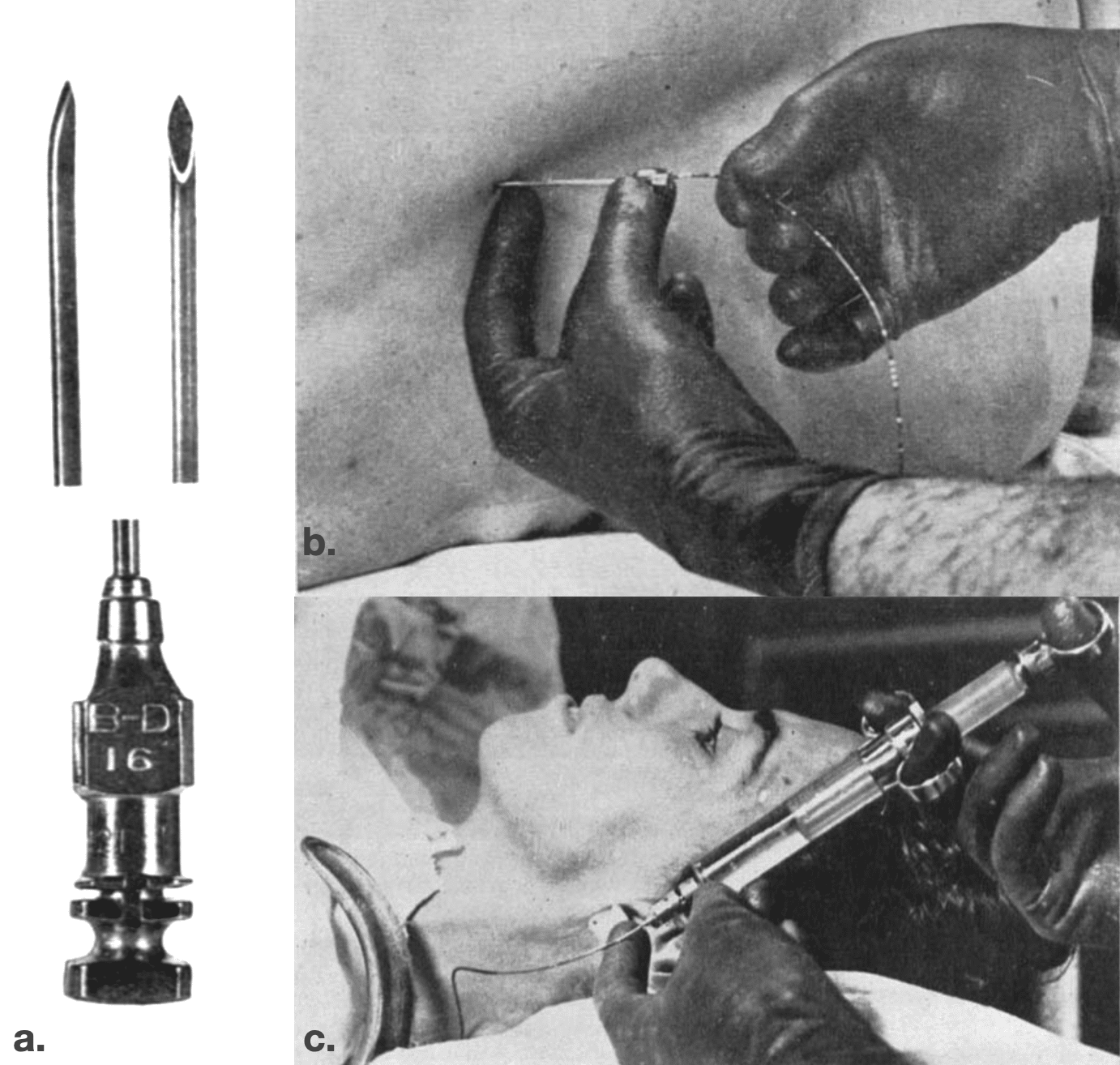
a. Tuohy needle with Huber point: Hub of needle (16 G)
b. Introduction of No. 3.5 catheter through the needle into the peridural space.
c. Fractional dose administration.
Modern epidural needle family
1950 – Flowers and the blunt-tip idea. Charles E. Flowers Jr (1920–1999), American obstetrician-gynaecologist, modified the Tuohy–Huber needle by blunting and slightly lengthening the Huber point, then adding a sharper stylet that projected beyond the needle tip. The design aimed to reduce dural puncture while allowing skin penetration, but the tip could bend, making stylet removal or catheter threading difficult. The Tuohy–Flowers needle itself was not successful, but the blunt-tip concept influenced later refinements.
1951 – Crawford needle. Oral Bascom Crawford Jr (1921–2008), American anaesthesiologist, developed a Quincke-type epidural needle with an extremely short, flat, blunt bevel. He used the bevel down to identify the epidural space, then rotated the needle 180° to direct catheter passage cephalad. Crawford favoured the hanging-drop method and, in 1951, published a large thoracic/cervical peridural series of 677 cases.
1961 – Weiss needle. Jess Bernard Weiss (1917-2007), American anaesthesiologist, modified the Tuohy–Huber needle for the hanging-drop technique by adding stabilising wings at the hub and blunting the tip. The wings allowed two-handed advancement while the operator watched the drop at the hub; the dulled tip allowed the dura to be displaced without perforation, helping generate the negative pressure needed for the hanging-drop sign.
1965 – Hustead needle. Robert Frank Hustead (1928-2008), American anaesthesiologist, refined the Tuohy–Huber needle by eliminating the secondary bevel, altering the bevel angle, shortening the needle opening, and smoothing the heel to reduce catheter trapping or shearing. The manufactured Hustead needle had an opening not exceeding 2.7 mm and a bevel angle of approximately 12–15°.
1957–1993 – Other epidural needle variants. Wagner, Cheng, Crawley, Foldes, Bell, Brace, Lutz, Scott and Eldor designs appeared as variations on the Huber-Tuohy or blunt-tip concept, with changes in bluntness, markings, hub design, pencil-point configuration, Luer-lock connection, or combined spinal–epidural use. The Cheng needle was notable as an early epidural needle with centimetre depth markings, while the Eldor needle was designed for combined spinal–epidural anaesthesia.

Catheter materials and modern design
1940s – Ureteral catheters and early continuous neuraxial access. Early continuous neuraxial techniques borrowed small ureteral catheters from urological practice. Love used a 5F ureteral catheter with a 13G Barker needle for subarachnoid drainage; Tuohy used a 4F lacquered silk catheter through a 15G Barker needle for continuous spinal anaesthesia; and Curbelo later used a 3.5F silk ureteral catheter through a 16G Tuohy needle for continuous lumbar peridural anaesthesia. These catheters made repeat dosing possible, but were awkward, relatively large, and difficult to sterilise reliably.
1949 – Plastic epidural catheters. Flowers, Hellman and Hingson described plastic tubing for continuous obstetric peridural anaesthesia in 1949. This was a major practical advance over silk or ureteral catheters: plastic tubing was easier to place, more reliable, cheaper, and better suited to routine obstetric use.
1950s–1970s – Polymer evolution. Early polyethylene catheters were followed by polyvinyl chloride, then later nylon, Teflon, polyurethane and silicone. These materials allowed manufacturers to produce thinner catheters with better kink resistance, tensile strength, stiffness, and handling characteristics. The catheter was no longer merely something passed through the needle but was designed as an essential component of the epidural system.
1990s – Tip, orifice and stiffness. Modern epidural catheter design focused on how the catheter behaves once inside the epidural space. Material stiffness, open- or closed-tip design, single- or multi-orifice configuration, radiopacity, tensile strength and resistance to kinking all affect placement, spread, migration, paraesthesia, intravascular cannulation, catheter breakage and removal. The endpoint of the epidural needle story is therefore not just a better needle, but a matched needle–catheter system.
References
Historical references
- Sicard A. Les injections médicamenteuses extra-durales par voie sacrococcygienne. Comptes rendus des séances de la Société de biologie et de ses filiales. 1901; 53: 396-398.
- Cathelin F. Une nouvelle voie d’injection rachidienne. Méthode des injections épidurales par le procédé du canal sacré. Applications a l’homme. Comptes rendus des séances de la Société de biologie et de ses filiales 1901; 53: 452–453
- Stoeckel W. Über sakrale Anästhesie. Zentralblatt für Gynäkologie. 1909; 33: 1–15.
- Läwen A. Über Extraduralanästhesie für chirurgische Operationen. Deutsche Zeitschrift für Chirurgie. 1910; 108: 1–43.
- Gil Vernet S. Nou procediment per anestesiar les arrels sacres. Anals de l’Academia i Laboratori de Ciències Mèdiques de Catalunya 1917;11:247-250
- Pagés F. Anestesia metamérica. Revista de sanidad militar (Madrid) 1921; 11(12): 351-365, 385-396
- Dogliotti AM. Un Promettente Metodo Di Anestesia Tronculare In Studio La Rachianestesia Peridurale Segmentaria 1931
- Aburel E. L’anesthésie locale continue (prolongée) en obstétrique. Bulletin de la Société d’obstétrique et de gynécologie de Paris. 1931; 20: 35-39.
- Soresi AL. Peridural anesthesia; a preliminary report. Medical journal and record 1932; 135: 165-166.
- Gutiérrez A, López–Rubido M. Resultados obtenidos con la anestesia peridural. Revista de cirugía de Buenos Aire 1933; 12: 93–101.
- Lemmon WT. A method for continuous spinal anesthesia: A preliminary report. Ann Surg. 1940 Jan;111(1):141-4
- Edwards WB, Hingson RA. Continuous Caudal Anesthesia During Labor and Delivery. Anesthesia & Analgesia: 1942; 21(6): 301-311
- Manalan SA. Caudal block anesthesia in obstetrics. Journal of the Indiana State Medical Association 1942; 35: 564–565
- Adams RC, Lundy JS, Seldon TH. Continuous caudal anesthesia or analgesia: a consideration of the technic, various uses and some possible dangers. JAMA. 1943; 122(3): 152–158
- Edwards WB, Hingson RA. Continuous Caudal Anesthesia in Obstetrics. JAMA. 1943; 121(4): 225-229.
- Southworth JL, Hingson RA. Continuous Caudal Analgesia in Surgery. Ann Surg. 1943 Dec;118(6):945-70.
- Tuohy EB. Continuous Spinal Anesthesia: Its usefulness and technic involved. Anesthesiology 1944;5:142-148
- Huber RL. Hypodermic needle. US Patent 2,409,979. October 22, 1946.
- Martínez Curbelo M. Continuous peridural segmental anesthesia by means of a ureteral catheter. Curr Res Anesth Analg. 1949 Jan-Feb;28(1):13-23
- Flowers CE Jr, Hellman LM, Hingson RA. Continuous peridural anesthesia and analgesia for labor, delivery and cesarean section. Curr Res Anesth Analg. 1949 Jul-Aug;28(4):181-9.
- Flowers CE Jr. A technique of continuous peridural anesthesia using a blunt needle. Curr Res Anesth Analg. 1950 Jan-Feb;29(1):39-42
- Flowers CE Jr, Hellman LM, Hingson RA. Continuous peridural anesthesia and analgesia for labor, delivery and cesarean section. Curr Res Anesth Analg. 1949 Jul-Aug;28(4):181-9.
- Flowers CE Jr. A technique of continuous peridural anesthesia using a blunt needle. Curr Res Anesth Analg. 1950 Jan-Feb;29(1):39-42
- Crawford OB, Buckingham WW, Ottosen P, Brasher CA. Peridural anesthesia in thoracic surgery; a review of 677 cases. Anesthesiology. 1951 Jan;12(1):73-84.
Eponymous term review
- Frölich MA, Caton D. Pioneers in epidural needle design. Anesth Analg. 2001 Jul;93(1):215-20.
- Goerig M, Freitag M, Standl Th. One hundred years of epidural anaesthesia—the men behind the technical development. International Congress Series, 2002; 1242: 203–212
- Aldrete JA, Cabrera HS, Wright AJ. Manuel Martinez Curbelo and continuous lumbar epidural anesthesia. Bull Anesth Hist. 2004 Oct;22(4):1, 4-8.
- Toledano RD, Tsen LC. Epidural catheter design: history, innovations, and clinical implications. Anesthesiology. 2014 Jul;121(1):9-17.
- Waurick K, Waurick R. Epiduralanästhesie – Geschichte und Technik der Epiduralanästhesie [History and Technique of Epidural Anaesthesia]. Anasthesiol Intensivmed Notfallmed Schmerzther. 2015 Jul;50(7-8):476-82
- Benhardt AC, Kodali BS. All epidural needle bevels are not the same. Indian J Anaesth. 2021 Apr;65(4):328-330.
- Bowers EGM. Born on the Battlefield: Celebrating the Centennial of the Discovery of Epidural Anesthesia. Mil Med. 2021 Nov 2;186(11-12):295-296.
- López Álvarez S, Casas Reza P, Del Río Fernández S. Centenary of epidural anaesthesia. Rev Esp Anestesiol Reanim (Engl Ed). 2022 Jan;69(1):4-11.
- Chinn GA, Gray AT, Larson MD. Overcoming Obstacles: The Legacy of Fidel Pagés, Founder of the Epidural, 100 Years After His Passing. Anesth Analg. 2024 Feb 1;138(2):475-479.
eponymictionary
the names behind the name

BSc MD, University of Western Australia (UWA). Medical interests in critical care, FOAMed and simulation training. Outside of medicine, I'm passionate about sport, camping and the outdoors.
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |
